|
 |
| Sunday, 28 September 2003 |
| Features |
| News Business Features Editorial
|
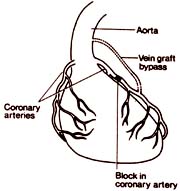
Today is World Heart Day Some recent techniques in heart surgery : Surgery for coronary artery disease Coronary arteries are the blood vessels which supply the muscle of the heart with its oxygen and energy supply. Coronary arteries can become blocked by the build-up of a fatty substance (atheroma) in the wall of the coronary artery. When the blockage is severe it produces chest pain during exercise and can produce a heart attack when some heart muscles die.
In coronary artery surgery procedures a bypass graft is carried out which allows the blood to flow from the aorta, the main blood vessel out of the heart, into the coronary artery beyond the site of the blockage. A bypass graft is created for each of the main coronary arteries affected by coronary artery disease. In some patients this will involve only a single graft to one affected artery. More commonly, two, three or four grafts are necessary.The surgeon uses another blood vessel from the patient's own body to create the graft. More often this is a vein removed from the leg. The leg vein which lies just underneath the skin may be removed safely without interfering with the health of the leg. In some patients, perhaps because of varicose vein problems in previous years, leg vein may not be suitable. It is then possible to use vein from the arm. In the last few years, it has become apparent that an artery which runs inside the chest wall, known as the internal mammary artery, can be used to create bypass grafts in coronary artery disease patients. Most surgeons now believe that when possible, this artery should be used, especially in younger patients, since the use of the artery graft gives excellent long-term results. When 3 or 4 grafts are required, the surgeon will use both the internal mammary artery and vein grafts. Coronary artery surgery procedures are, as with valve operations, carried out through the same chest incision, using heart/lung bypass during the operation. Risks Hospital mortality (death within 30 days of the operation) is low, around 2 per cent, for many procedures. This is a very low risk figure and indicates the tremendous success of this type of surgery. The risk is greater in patients whose heart muscle has previously been severely damaged by major heart attacks. Over 15,000 patients have coronary surgery procedures in the UK each year. ########### Surviving heart attacks In Sri Lanka, the patients belonging to lower socio-economic classes usually have a poor survival rate and higher mortality (death) rate than the rich when they get serious heart attacks and heart failure as the rich patients always have an easier access to (a) the family physicians (b) specialists and (c) private nursing homes with intensive care facilities. There is no doubt that our government hospitals are manned by very highly qualified and experienced specialists and these hospitals have fully equipped intensive care units (ICUS) manned by experienced and very devoted staff.
But the main problem faced by most of the major hospitals is that the ICU facilities available at present are not sufficient for the large number of seriously ill heart patients admitted to these major hospitals. It is common knowledge that any patient suffering from severe angina or acute myocardial infarction (heart attack) should be admitted to an intensive care unit (ICU) where the patient has access to life-saving drugs (such as streptokinase) and where facilities for monitoring of heart rhythm are available. Thrombolytic drugs such as streptokinase should ideally be administered in an ICU and these clot-dissolving drugs if administered to heart attack patients in the first six hours of the heart attack, reduces the cardiac muscle damage and lowers the mortality rate of heart attack patients. It is only in an ICU that a heart attack patient getting a cardiac arrest can be successfully resuscitated.
Take the example of a poor person in Kataragama or Madulsima or Thanamalwila getting a serious heart attack. By the time the patient gets admitted to a base hospital or a provincial hospital, the patient would be dead or if alive, there will be significant cardiac muscle damage and the patient will be a permanent cardiac invalid even if the patient has the luck to leave the hospital. Majority of heart attack (and strokes) occur during the night. It is a fact that some of these heart attack patients admitted to government hospitals especially during the early hours of the morning are not examined by a specialist due to various reasons and mortality is highest during the night. These patients are very often examined by the consultant physician during the next morning ward round. Of course, there are exceptions to the above rule especially in the University medical units where the very ill heart patients are examined by a specialist during the night. Well-to-do patients who get heart attacks at night on the other hand are generally admitted to ICUS of nursing homes as they are almost sure of being examined by a specialist. In contrast, the poor heart attack patient who gets admitted to a major government hospital may not get ICU treatment as the ICU facilities in most of the government hospital is limited. Majority of heart attack patients admitted to government hospitals are treated in the ordinary medical wards and are transferred to the ICU if the patient gets a serious cardiac complication such as severe angina, serious cardiac rhythm problem, low blood pressure (cardiogenic shock) or heart failure. Urgent biochemical tests There are certain urgent biochemical tests that should be done in all cases of severe angina and heart attacks. Troponin-T and cardiac enzyme including CK and CPK (mb) estimation are two such tests which help the physician to diagnose acute coronary syndrome and myocardial infarction accurately before the ECG shows abnormalities especially in cases of patients with severe angina with normal ECG Troponin-T helps the physician to separate out the patients whose Troponin-T is positive and observe these very ill patients in the ICU even if the ECG does not show definite changes of ischaemia or infarction. It is very unfortunate that this urgent and very useful test cannot be done in our government hospitals including the National Hospital, Sri Lanka (NHSL) which gets a large number of heart attack patients daily. In the majority of private nursing homes and private labs Troponin-T can be done and the results are available in about 20 minutes and it costs the patient about Rs. 1100 to Rs. 1300 for the test. Estimation of cardiac enzymes This is another extremely useful biochemical test that should be done in all patients with heart attacks. As mentioned previously there are heart attack patients with almost normal ECG and with abnormal cardiac enzymes who have to be monitored in the ICUS. Estimation of cardiac enzymes cannot be done in our government hospitals. As thrombolytic (clot-dissolving) drugs such as streptokinase have to be given within the first few hours of getting a heart attack, the results of the cardiac enzymes estimation should be available to the physician as early as possible as there are certain heart attacks where ECG on admission does not show confirmatory evidence of myocardial infarction. The results of this test can be obtained in private hospitals and private labs in about half an hour and the patient has to spend about Rs. 1100 to Rs. 1500 for the above test. NHSL is the only state hospital where this test can be done at present. I understand that it takes a few hours for the lab to release the report. When the heart attack patient's blood is sent to the NHSL lab, in the night I am told that the report is available only next morning by which time it does not serve much of purpose.In case of rich patients admitted to ICUs of government hospitals, the usual practice is for the ICU staff is to hand over a blood sample for cardiac enzymes and Troponin-T to the patients guardian to get the test done in a private lab. At present majority of myocardial patients admitted to government hospitals are treated without getting the above biochemical tests. It is the duty of the health authorities to arrange for the introduction of these very important tests at least to the teaching hospitals, provincial hospitals and base hospitals so that lives of a large number of heart attack patients could be saved. The elderly heart attack patients have a very poor prognosis (prospect of recovery) when they get heart attacks and very often they are a neglected lot, both in patients home as well as in the hospital. This applies to both the rich and the poor. Coronary artery surgery Coronary artery surgery (CABG) and angioplasty (P.T.C.A.) for patients with severe angina (unstable angina) and myocardial infarction has to be performed without delay. The government patients who need above procedures are usually given a date in the waiting list for coronary angiography and another date in the surgical waiting list for CABG and some very ill patients who need urgent CABG might die while awaiting for above procedures. Coronary angiogram costs about Rs. 30,000 and CABG costs about another Rs. 275,000 in the private sector. A patient belonging to the lower socio-economic class cannot afford CABG in a nursing home.To conclude patients with lower income more often have greater co-morbidity and mortality than those of greater means. ***** How a heart disease starts
***** Coronary angioplasty Coronary angioplasty is a relatively new technique for treating coronary artery disease. The first procedure was done in 1977 and development has been rapid since then. Patients with angina usually have narrowings or blockages in one or more of the three main coronary arteries. The idea of coronary angioplasty is to pass a very fine catheter down the coronary artery and across the narrowed or blocked section. A sausage shaped balloon, mounted on the end of the catheter, is then inflated which stretches the vessel and compresses the material blocking it. When the balloon is deflated and removed an enlarged channel remains which permits improved blood flow to the heart muscle. Although it sounds simple, angioplasty is technically demanding. From the patient's point of view the procedure is very similar to cardiac catheterisation though it may take much longer to manipulate the balloon catheter into the right spot. Anginal symptoms during balloon inflation are common but not invariable - the pain eases when the balloon is deflated. At the moment only about one-third of the patients having a catheter test for angina are suitable for angioplasty. The reason for this is that in many patients the blockages are too numerous, too tight or too long for our current technology to cope with. The technique can also be used in patients with previous by-pass graft surgery if the graft has become narrowed. Complications Most angioplasty procedures are uncomplicated. Sometimes, however, the treatment completely blocks off the artery which was previously narrowed. If this happens and the doctor thinks that serious injury to the heart will result, he may ask a surgeon to perform an immediate bypass graft operation. Patients undergoing angioplasty must therefore understand that they may end up having an urgent operation and be prepared for this. The illustration is a diagrammatic representation of a typical angioplasty procedure. Note that the sausage shaped balloon does not blow up to more than 2 to 3 mm. in diameter. (British Heart Foundation) ############### Coronary angioplasty Coronary angioplasty is a relatively new technique for treating coronary artery disease. The first procedure was done in 1977 and development has been rapid since then. Patients with angina usually have narrowings or blockages in one or more of the three main coronary arteries. The idea of coronary angioplasty is to pass a very fine catheter down the coronary artery and across the narrowed or blocked section. A sausage shaped balloon, mounted on the end of the catheter, is then inflated which stretches the vessel and compresses the material blocking it. When the balloon is deflated and removed an enlarged channel remains which permits improved blood flow to the heart muscle. Although it sounds simple, angioplasty is technically demanding. From the patient's point of view the procedure is very similar to cardiac catheterisation though it may take much longer to manipulate the balloon catheter into the right spot. Anginal symptoms during balloon inflation are common but not invariable - the pain eases when the balloon is deflated. At the moment only about one-third of the patients having a catheter test for angina are suitable for angioplasty. The reason for this is that in many patients the blockages are too numerous, too tight or too long for our current technology to cope with. The technique can also be used in patients with previous by-pass graft surgery if the graft has become narrowed. Complications Most angioplasty procedures are uncomplicated. Sometimes, however, the treatment completely blocks off the artery which was previously narrowed. If this happens and the doctor thinks that serious injury to the heart will result, he may ask a surgeon to perform an immediate bypass graft operation. Patients undergoing angioplasty must therefore understand that they may end up having an urgent operation and be prepared for this. The illustration is a diagrammatic representation of a typical angioplasty procedure. Note that the sausage shaped balloon does not blow up to more than 2 to 3 mm. in diameter. (British Heart Foundation) ################ After heart surgery Going home is the next step on the road to recovery following heart surgery. These guidelines have been written to anticipate most of the questions that are likely to crop up over the next few weeks following surgery. Recovery from the operation will take about three months for most patients. Remember that after the operation your heart is stronger and in a better condition than when you came into hospital, be confident that you are a new person. Do not regard yourself as a "Heart Patient" any more. For most heart operations the breastbone is divided, and therefore will take a number of weeks to heal properly. During this time (up to 6-8 weeks or longer) it is common to experience aches and pains in the chest, shoulders, back and neck. A mild painkiller e.g. Panadol, (Paracetamol), Panadine should be taken to relieve this. If this is not adequate, you may need to consult your family doctor for more stronger tablets. Lifting: As your breastbone is healing, you must be careful not to put it under undue strain. Avoid lifting, pushing or pulling heavy objects for about 3 months; also awkward reaching and straining. Use both hands and turn to face what you are trying to move. Rest: You will probably feel weak initially and tire quickly. Take care to build things up gradually with plenty of sleep including an afternoon nap if needed. Exercise: Your heart is in a better condition now and it needs to do work to get back into normal activity. You should try to get out walking daily. Try to gradually increase the distance you walk, but do not overdo it if you are becoming tired or short of breath. Many people are walking up to a mile a day after 6-8 weeks. Exercise will help you and your heart get fitter if carried out carefully and sensibly. Sexual Relationships: These may be resumed when you feel ready. You and/or your partner may feel apprehensive initially - this is perfectly normal. Try to choose a comfortable position that does not put too much pressure on your chest initially - a less active role is preferable - and do not be afraid to discuss your fears with your partner. Avoid intercourse soon after a heavy meal and try to find a time when you feel rested and relaxed. Work: Many people return to work about three months after surgery. This will depend on your recovery after the operation and the nature of your job. If you are doing a "desk" job, you may be ready to go back after 2 months. For those having strenuous jobs - a full 3 month is advisable. Driving: You are not permitted to drive for at least one month following heart surgery. Check with the doctor before resuming driving. Stress: Try to avoid stress as much as possible. If you are the kind of person who becomes tense and anxious under the pressures of work or domestic life you will put a strain on your heart. Practice relaxation exercises to help you learn to relax. Meditation is extremely beneficial. If your blood pressure was high before the operation, make sure your Cardiologist checks it regularly afterwards. Smoking: This is detrimental to your health and in particular your heart. Smoking speeds up the process of "furring" of the arteries and if you continue to smoke you can block up your grafts. You must stop smoking immediately. Alcohol: Alcohol in moderation is permitted. Try to have a couple of days each week free from alcohol. Large volumes of alcohol should not be taken with strong painkillers or if you are taking warfarin. It is best for your general health to stop alcohol completely. Diet: If a particular diet has been advised, you must stick to it. In general a healthy diet means trying to increase your fibre intake and reducing the amount of fat (particularly animal fat) sugar and salt. If you have had coronary artery bypass surgery, make sure you (and your family) have your cholesterol level checked by your doctor and followed up if they are found to be high. It should be reduced by diet and/or tablets. Hygiene: You are able to take a shower/bath once your wound is dry and healing. Wash gently around the wound site and dry it. Wound: If you develop a temperature or notice any redness, tenderness or discharge around the wound site, consult your doctor. Eyesight: You may find that your vision is not as sharp in the initial stages after the operation. This is due to pressure changes in the eyes around the time of surgery and will usually resolve. People wearing glasses may find that their vision is variable and their glasses do not seem to work as well as they did before. This is a temporary situation and it is therefore inadvisable to consider having your glasses changed in the first 4-6 weeks after surgery. Infection: If you have a temperature or any sign of infection it is important to see a doctor and remind them that you have had a heart valve replaced. There is a small possibility of the infection being related to the valve. Dentist: It is important for anyone with a valve replacement to have regular (6 monthly) dental checks because of the possible risk of infection. Make sure your dentist knows you have had a heart valve replacement - any extractions must be covered with antibiotics. Do not forget to inform your dentist if you are taking warfarin. Yearly check-ups are important to maintain your general health. Ideally, you should have a yearly check-up by your doctor, this should include blood pressure, Urine sugar and Cholesterol level. Courtesy: New Nawaloka Hospitals (Pvt.) Ltd. |
|
News | Business | Features
| Editorial | Security Produced by Lake House |