 |
 |
| Sunday, 8 February 2004 |
| Features |
| News Business Features Editorial
|
Compiled by Carol Aloysius The Silent Thief
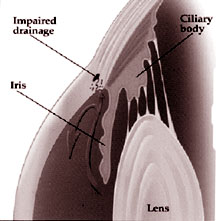
Q: What is Glaucoma? A: The eye has its own internal "plumbing" system that circulates a fluid called aqueous through the eye around the human lens and iris (colored circle of the eye). Aqueous nourishes the front parts of the intern eye and helps to maintain normal pressure which is needed for the normal shape and function of the eye. This aqueous has nothing to do with tears produced by the eye. Aqueous is constantly produced by the ciliary body in the eye and drained out via the angle of the eye in to the general blood stream. When something goes wrong with this plumbing system-usually because of drainage system block or too much fluid build up in the eye, the intraocular pressure raises. This high pressure produced due to the imbalance the amount of fluid produced and the amount drained out, puts a strain on the delicate nerve structures in back of the eye called the optic nerve. The optic nerve is like an electric cable containing a million wires. Each wire or "nerve fibre" carries messages to the brain and these messages join together and interpreted as vision by the brain. Glaucoma can damage these nerve fibres, causing blind spots to develop. Q: Why is it called a "Silent Thief" A: Most glaucomas do not have obvious symptoms except during advanced stages of the disease and in case of acute attacks. The vision loss begins in the peripheral circle around us and finally encroaches the centre by which time disability is permanent. Hence the term "Silent Thief" - You lose without Knowing!! Q: Who are more likely to develop glaucoma? A: Persons over 35 years of age; Blood relatives of glaucoma patients; Very near sighted persons (myopes); People with diabetes mellitus. It is a must for everybody above 35 to have a yearly eye exam that includes measurement of eye pressure and fundoscopy to check the optic nerve. Q: What causes glaucoma? A: In most cases of primary glaucoma, there is no identifiable cause except a possible hereditary predisposition. The basic shape of the eye may predispose some people to develop some types of glaucomas. Q: Are there different types of Glaucoma? A: Yes. There are many different kinds of glaucoma. . Primary open angle glaucoma: This occurs when the drainage angle simply become less efficient causing a gradual increase in the pressure. If this increase in pressure is sufficiently high to cause optic nerve damage it is known as "primary open angle glaucoma" or "chronic open glaucoma." It is much prevalent in adults particularly above 35 years of age. There may be a hereditary tendency. Most people who have chronic glaucoma feel normal and have good central vision. People seldom notice the blind areas that develop in periphery until considerable optic nerve damage has already occurred leading to a condition called "tunnel vision". Fortunately, this form of glaucoma progresses slowly and responds well to eye drops and/or tablets. These medicines either decrease the aqueous production or they increase the outflow of aqueous from the eye. . Primary angle closure glaucoma: Some time the drainage of the eyes suddenly becomes blocked. It is as though a sheet of paper floating near the drain suddenly drops over the opening and blocks the out flow. In the eye the sheet of paper is the iris. In some eyes there is less space between the lens and the iris. Certain factors can precipitate the sudden blockage of these narrow spaces. The eye pressure usually increases rapidly resulting in various symptoms of Acute angle closure glaucoma namely, Blurred vision - Rainbow haloes around light - Severe pain - Nausea and vomiting - Head ache. Unless the ophthalmologist diagnoses and treats this condition early, blindness can result. Treatment for angle closure glaucoma involves laser therapy (peripheral iridotomy) or microsurgery to remove a small portion of bunched up iris (peripheral iridectomy). Many a times the iris may block the angle gradually as if a zipper is closing the angle. This leads to a gradual and painless closure of the angle is called chronic angle closure glaucoma. . Low tension glaucoma or normal tension glaucoma: This is a puzzling form of glaucoma. In some cases, a person begins to suffer optic nerve damage even though the fluid pressure in the eye is in the normal range. Recent studies suggest that the problem may be related to hardening of the arteries that supply blood to optic nerve. Medications to bring the eye pressure down even below normal level seem to be the best way to control this condition. Secondary glaucomas: These occur when the drainage angle is damaged by specific conditions like injuries, certain drugs (steroids), tumors, advanced cases of cataract, diabetes or inflammation. Treatment is directed to the basic problem in addition to the glaucoma. Congenital or developmental glaucoma: This is a very rare condition affecting infants/young people. This may be inherited and may be a result of incorrect or incomplete development of the eye's drainage channels during growth of the child in the mother's womb. The parents may notice in their baby . Enlarging eyeball The infant or child should be taken to an ophthalmologist immediately. Detailed evaluation would usually mean examination under general anaesthesia. Q: How is glaucoma diagnosed? A: There are 4 factors based on which glaucoma is diagnosed. . Intraocular pressure (IOP) Tonometry: is used to measure the intraocular pressure. Normal intraocular pressure ranges from 12 to 22 mm of Hg (millimeters of mercury). Applanation tonometry is the most standardized measurement technique. Ophthalmoscopy: is used to examine the inside of the eye especially the optic nerve. The normal optic nerve is healthy pink colour with a small depression in the centre of the disc called as "optic cup." Due to increase in the intraocular pressure there may be an enlargement in this cup secondary to damage to the nerves. Any enlargement of the optic cup or an asymmetry between cups of the two eyes may suggest glaucoma. Gonioscopy: is a very important test to check whether the angle of the anterior chambers i.e. the angle where the iris meets the cornea is open or closed. This helps in differentiating between various types of glaucoma and to adopt appropriate treatment measures. Perimetry: is a special test to map the complete field of vision. Glaucoma damage first occurs as a slight change in the field of vision. These small changes in the field of vision can be detected and quantified by computerized perimetry which not only allow an accurate assessment of the visual field but also helps in subsequent follow up. Slip lamp examination; This is a microscope that magnifies and illuminates the cornea and iris and aids the doctor in finding conditions that may cause secondary glaucomas. A diagnosis of glaucoma is not always possible on one single evaluation. On occasions multiple evaluations may be needed before confirming the diagnosis. The decision to treat is also based on many tests and not only on the intraocular pressure recording. Q: Can glaucoma be cured? A: In most situations, glaucoma is controlled but not cured. i.e., it needs constant monitoring of vision, intraocular pressure, fields and optic nerve head to titrate the treatment. Hence, there is tremendous responsibility on the part of the patients to have a regular follow up and to religiously follow the instructions. Q: How is glaucoma treated? A: There are 3 modalities of treatment 1. Medicines, 2. Laser, 3. Surgery. Q: Medications: A: 1. Eye drops, 2. Oral tablets. They may either increase the drainage of fluid out of the eye or decrease the production of fluid in the eye. Glaucoma medications come in many different strengths and combinations. Doctors try to use the least amount of medication that produces the best result with the lease side effects. Most medications have some but usually tolerable side effects. These usually become less noticeable after few weeks of use. If the side effects are too uncomfortable or continue too long, doctors often change to a lower dosage of some medications or switch to another medication. Can glaucoma be treated with laser? A: Yes. Laser is a tiny powerful beam of light that can make a small burn or opening in a tissue depending on the strength of light beam. Usually laser treatments are performed as outpatient procedures. Two modalities of laser are commonly employed: 1. Peripheral iridotomy - (P.I.) In this procedure a hole is created in the iris to relieve the block that occurs in acute angle closure glaucoma. Very often the fellow eye is also treated to prevent the acute attack, even if patient is symptomatic in one eye. 2. Argon laser trabeculoplasty (A.L.T.): This treatment is used to treat chronic open angle glaucoma to help improve the drainage facility. It is usually done in addition to use of eye drops. Microsurgery: Surgery may be the last resort in most cases of open angle glaucoma (angle closure) if medication/laser are unable to control the disease. In congenital glaucomas, surgery may be the first option. Surgery is usually performed under local anaesthesia. General anaesthesia may be required in infants and young children. Trabeculectomy is the most commonly performed surgery in glaucoma. during this procedure a small partial thickness portion of the sclera (white part) of the eye is removed along with the small peripheral portion of the iris. In this procedure the new opening so created allows the intraocular fluid to bypass the clogged drainage canals. After surgery the area over the site of surgery looks like a blister or bubble - called a bleb. Glaucoma microsurgery is usually successful, but occasionally the new drainage canal may begin to close and the pressure may rise again. This can happen because of the body's natural tendency to heal the new opening in the eye. This is more common in younger patients who have stronger capabilities compared to older people. Q: Can a patient of glaucoma have cataract? A; Yes, since glaucoma usually occurs in older individuals there may be associated cataract. Occasionally your doctor may suggest you to have cataract and glaucoma operation at the same time. What can be the complications of surgery? In a majority of the cases, surgery is successful. Problems that may include 1. Excessive filtration in which case the eye may be comparatively soft. However, only in a small percentage of cases, it is significantly low as to affect the vision. Additional treatment may be needed in such cases to reduce filtration. 2. Haemorrhage: one of the very rare but significant complications is uncontrolled bleeding in to the eye. On occasions such a complication can result in permanent and significant effect on vision. 3. Infection: Since a communication is established between the inside of the eye and outer layers of the eye, the potential for infection exists even long after the surgery. General precautions that should be followed are: a. Never rub the operated eye. b. In case of pain, redness or discharge, immediately seek opinion of eye specialist. It may be advisable to keep a bottle of unopened antibiotics eye drops in your house. In case of symptoms are explained earlier, you can instill these drops every hour in the affected eye and visit the local eye specialist immediately. Helpful suggestions: . Use medications regularly, maintaining appropriate time intervals. ************* Nutrition for the mother and child by Prof. T. W. Wickramanayake, Nutrition Society.
It is also a period when the child develops diarrhoea and other infections. The care givers should wash their hands well before food preparation and feeding, and the child's hands washed before eating. Food should be offered soon after preparation and served in clean cups and bowls, not feeding bottles. Breast feeding should be continued throughout the 24 months, to ensure an intake of protective substances, of good quality protein and of micro-nutrients. A mother leaving home for work can give at least 3 breast feeds a day. One early in the morning, one in the evening and the third at bed time. If the child cries in the early hours of the morning a fourth meal could be given. Complementary foods given in the first few months should be well cooked and soft, offered frequently and with a great deal of patience. It takes time for the child to change from the suckling process to one of chewing and swallowing. A combination of cereals, pulses, animal foods, vegetables and fruit should be presented, increasing the portion size as the child gets older. The timing of meals and snacks is important. The child's stomach is small and empties quickly. Small means at frequent intervals will be preferred to large meals three or four times a day. A small child should not be expected to adopt an adult's feeding pattern. The average pre-school child consumes food 4 to 7 times a day. Older children should be offered food at intervals of at least 4 hours, not more frequently than 2 1/2 hours. Parents should remember that they determine the choice of food that will be eaten by a child, as children tend to imitate the feeding patterns of their parents. Non-nutritive foods play an important role in children's attitude to food. Withholding foods as punishment and offering foods as rewards or as a measure of affection, distorts the value of such foods and makes them more desired or preferred. The quality of food offered also influences its acceptance. Children like well prepared foods, attractively served. They prefer mild flavours and enjoy preparations that can be easily chewed. The emotional climate at meal time influences appetite and food consumption. Battles between parents or with children should not be waged at the dinner table. Fatigue and excitement also dull the appetite. A complementary meal could be prepared as follows: Ingredients Uncooked, under milled rice 40g, uncooked pulse 15g, yellow vegetables (yellow pumpkin, carrot), dark green leafy vegetable 40g, oil or fat 5g. The pulse (say, green gram) should be soaked overnight, the seed coat removed, and cooked until soft, well mashed and fed in small quantities at a time with the boiled rice. The leaf (spinach, sweet potato, thampala or kankun) should be cut up into small pieces and cooked with the rice. The pumpkin or carrot should be well boiled and mashed with the rice. The fat or oil will improve the consistency of the rice gruel and also reduce the amount of water needed to keep the mixture semi-solid. The food is given after a breast feed. A small amount of animal food could be added to enhance the quality of the meal, the meat or fish being well cooked and shredded, minced or chopped. Small dried fish (such as sprats), washed and well dried, could be powdered, sieved to remove large pieces of bone, and stored in a dry bottle. Small amounts of the powder could be added to the rice that is being cooked. The green gram could also be powdered and stored, after removing the seed coat. The following are some guidelines every new mother should follow to ensure good health for her child. 1. Continue breast feeding as often as possible, till the child is 24 months old. 2. Continue visiting the clinic, having the child's weight marked on the growth chart. If the child moves away from his/her growth channel and the weight does not keep increasing steadily, consult the doctor. 3. Introduce complementary foods in the sixth or seventh month, increasing the quantity fed as the child gets older. 4. Increase feeding frequency after the 9th month, using a combination of meals and snacks. 5. Gradually increase food consistency and variety, adapting the diet to the infant's requirement and ability. Make the transition to the family diet during the 12th month. Food from the family pot should be taken off before ingredients such as curry powder and chillies are added. 6. Diversify the diet to improve quality and micronutrient intake. 7. Practise active feeding. Feed slowly, with patience, minimizing distractions during meals. Talk to children during feeding. Assist older children to feed themselves. 8. Practise fregnent and active feeding during and after illness. 9. Always practise good hygiene and proper food handling. |
|
News | Business | Features
| Editorial | Security Produced by Lake House |

 High eye pressure often goes unnoticed. By the time it is detected it
has already caused some vision loss. In Sri Lanka the number of patients
with Glaucoma is on the rise. Dr. Arun Narayanaswamy of the Apollo
Hospitals, Colombo, a specialist in Glaucoma (eye pressure) speaks to
Carol Aloysius of the disease that creeps on you unawares like...
High eye pressure often goes unnoticed. By the time it is detected it
has already caused some vision loss. In Sri Lanka the number of patients
with Glaucoma is on the rise. Dr. Arun Narayanaswamy of the Apollo
Hospitals, Colombo, a specialist in Glaucoma (eye pressure) speaks to
Carol Aloysius of the disease that creeps on you unawares like...
 This is a period of transition, when a child moves from exclusive
breast feeding to a varied diet of solid foods. Foods added to a diet of
breast milk are referred to as complementary foods. Rates of malnutrition
tend to peak during the second six months of life, during which the infant
is learning to eat.
This is a period of transition, when a child moves from exclusive
breast feeding to a varied diet of solid foods. Foods added to a diet of
breast milk are referred to as complementary foods. Rates of malnutrition
tend to peak during the second six months of life, during which the infant
is learning to eat.




