 |
 |
| Sunday, 8 August 2004 |
| Features |
| News Business Features Editorial
|
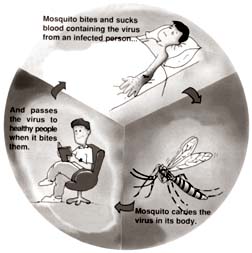
Clinical presentation of dengue virus infections The dengue epidemic has reached an all-time high. The grave complications following this disease could be avoided if the symptoms of dengue are detected early and accurately, says Dr. Rani Gunawardene in an interview with Carol Aloysius.
A: Most cases are probably asymptomatic without fever or with minimal symptoms. The symptomatic dengue virus infections can present with a wide range of clinical manifestations - from a mild febrile illness to major life threatening Dengue Haemorrhagic Fever (DHF) or Dengue Shock Syndrome (DSS). Q: What are the factors that influence disease severity ? A: Viral factors; DHF is highest with the serotype 2 dengue virus. . Prior Dengue infection: Infection with one of the four serotypes causes life long immunity. An individual can be infected four times with the four serotypes during a life time. Studies have shown that the severity of the DHF/DSS is more in secondary dengue virus infection. . Age: After the age of 19 yrs the severity of DHF declines. In endemic areas the high risk of DHF is seen in infants and those between six and 12 months. Q: How is Dengue fever diagnosed? A: Clinically, or by doing serologic and virologic test that will show virus or antibodies to the dengue virus. Q: Can the symptoms be missed even during a clinical diagnosis? A: Dengue virus infections may present with symptoms, which is more common, or without symptoms which is rare, and seen mostly in children where the presentation is asymptomatic, without fever or with minimal symptoms. Q: Can dengue virus infection present without high fever? A: Yes; In case of children with acute DF; In dengue primary infections. Fever may also be absent during a short period in classic DF between the first bout of fever and the second phase of fever. (saddle back) fever. In DHF there may be a period without fever. During this time between the 3-7th day Plasma leakage can occur leading to shock. DSS Q: What is Classic Dengue Fever (DF)? A: An acute illness accompanied with high fever (lasts for 5-7 days) may show a saddle back fever pattern; headache pain behind eyes (retro bulbar pain) body, bone, muscle pain joint pain (Break bone fever). In Children 19 yrs and less the classic DF picture is not seen. In children Gastro Intestinal and respiratory symptoms dominate. Interestingly most children with DF never develop typical symptoms. Q: What are the Gastro Intestinal Symptoms in DF? A: Anorexia (distaste for food), altered sensation of taste, nausea vomiting, diarrhoea, abdominal pain (mimic appendicitis) Q: What are the Respiratory Symptoms? A: Cough, sore throat, (redness of the throat (pharyngeal erythema) and nasal congestion (Mimic Bronchitis). Q: When does a rash appear during DF? A: Mostly seen in primary dengue infections and in females. The reddish maculo/papular rash appears on the 3-4th day after the fever begins and is seen on the torso from chest/back/abdomen to the arms and face, a second rash may appear later in the disease, and can be mistaken for Measles or Rubella. Q: Is DF easily detected in children? A: In children DF may take a milder form and is indistinguishable from influenza, Measles or Rubella. The acute phase is about one week followed by one to two weeks of convalescence with weakness, malaise and Anorexia. Q: What are the unusual manifestation of DF ? A: Heart; Myocarditis, irregularity in pulse with ECG changes. Lungs; Effusion; Liver failure; Abdomen ascites (fluid); Central Nervous System Dysfunction, Lethargy, Coma. Fits (seizures) Encephalopathy: Q: What are the Laboratory findings typical of DF? A: Low White blood cell count (leucopenia) Normal, low platelet count, abnormal liver function tests. Q: What is the treatment for dengue ? A: There is no specific therapy for treatment of a dengue infection. Q: What medicines can one take for fever? A: Analgesics (pain relievers) with acetaminophen only sparingly, and avoid those containing aspirin, and non steroidal inflammatory agents as there is a risk of Reye's Disease in children and bleeding. Patients should also rest and drink plenty of fluids to avoid dehydration. DF will resolve in 5-7 days. The most important measure is to continually assess the patient for impending complications like DHF. Q: What is Dengue fever with haemorrhagic manifestation ? A: Bleeding from nose (epistaxis) gums, gastro intestinal bleeding, can vomit blood, (haematemesis) pass blood in the stools (Malena) or can bleed, under the skin (purpura) petichae increase menstrual bleeding. In rare cases can develop intravascular coagulopathy. Q: What test is used to elicit haemorrhagic tendency ? A: Tourniquet test. Q: What is the treatment for DF with harmorhagic manifestations ? A: Blood Transfusion, Platelet Transfusion Q: What is Dengue Haemorrhagic Fever? A: It is a potentially deadly complication of DF. Q: What are the significant manifestations of DHF? A: High fever; fever as high as 40 to 41 degrees centigrade, fits, increased vascular permeability plasma leakage leading to pleural effusion and ascites and Dengue Shock Syndrome (DSS). Q: When does DSS occur? A: Between 3-7 days after the onset of the disease. Q: What are the signs and symptoms of DSS? A: Fever may be absent at this time. Abdominal pain may precede leakage of plasma in to the abdomen (ascites); Rapid weak pulse; Narrowed pulse pleasure less than 20 mm of hg (difference between systolic and diastolic pressure; Cold clammy extremities; Sweating; Skin may be blotchy and congested. Q: What are the clinical laboratory findings in DHF/DSS A: Low platelet count; Increased haematocrit value (PCV); abnormal liver function test; hypoproteinaemia. Q: What is the treatment of DHF/DSS? A: Oral and intravenous fluids, blood and platelet transfusion. Q: How does one identify and assess the high risk patients for shock and other complications? A: Duration of illness-maximum risk of shock is between 3-7 days of illness, with the resolution of fever 24 hours before and after. Haematocrit; increase in value of PVC warranting urgent fluid replacement; Low platelet count; abnormal liver function tests. If the above are normal the patients can be assessed daily at dengue clinics and referral to hospital is done only if the following signs are positive; Blood pressure less than 90/60 mmhg: Haematocrit more than 50 per cent. Platelet count less than about 50,000/mm3 evidence of bleeding other than petichae. When dengue virus is suspected on clinical grounds the patients should be treated empirically as appropriate for the sign and symptoms Q: Finally, how can travellers protect themselves from dengue? A: Apply insect repellent to exposed skin; Wear long sleeved shirts and
pants when out doors; Spray clothing with repellents as some mosquitoes
bite through the clothing; Use mosquito net if room is not
air-conditioned. Healthy diets start in the womb A mother's poor diet during pregnancy can cause her child to develop heart disease and diabetes in later life. Christine Doyle reports on the evidence that took scientists by surprise. For more than 10 years, Professor David Barker, Director of the Medical Research Council's Environmental Epidemiological Unit at Southampton University, has warned that heart attacks in adult life could result from poor development in the womb. His studies startled scientists, many of whom were sceptical. But subsequent research is proving him right. Prof Barker's thesis - that men and women who are small at birth and during infancy tend to have more coronary heart disease and strokes later in life - has growing support. Such people are also more likely to develop diabetes, have raised blood pressure and thinner bones. Of course, genes influence our health, and so, as we are constantly reminded, do rich, fatty foods, lack of exercise, smoking and being overweight. Yet, if Prof Barker's ideas are correct, how well a baby grows and matures in the womb and during infancy has a major impact on adult health, even up to 60 years later. Everything that helps the baby to develop in the womb comes from the mother, and, says Prof. Barker. "many women are not aware of the potential health risks". In his first book for the public, which he is writing now, Prof Barker says that women who are pregnant or thinking of having a baby must be more strongly warned about "the overriding importance of eating a well-balanced, healthy range of food, both during pregnancy and before". A poor nutritional start in the womb cannot automatically be put right after birth. Thin, light babies, who put on weight slowly or are undernourished, are also more likely to be more vulnerable to ill health later on. Yet an understandable inclination to overfeed such babies - to help them catch up or compensate rapidly for poor rations in the womb - could also cause problems. Prof. Barker explains: "Most organs are fully developed at birth; later on, they merely enlarge. Poor nutrition in the womb can lead to lifelong impairment in the ability of organs or tissues such as the heart, kidneys and muscle to function properly, especially if the body is challenged by obesity, inactivity or stress."
Epistaxis Bleeding from the nose is common in young and the old. Dr. Fazeenah Hameed explains some causes for this condition. Epistaxis or Rhinorrhagia is bleeding from the nose. Although there are various symptoms or states, most of the time they feel a burning sensation in the nostril, inflammation and itching. Blood flows drop by drop from one or both nostrils, sometimes blood starts to flow from succeeding orifices. Nose bleeding may be longstanding or short period, mild or severe, and unilateral or bilateral. Site of bleeding Little's area or Kiesselbach's plexus . Commonest site of bleeding is the Antero - inferior part of the nasal septum which is a highly vascular area making the anastomosis between the branches of various blood vessels supplying the nose. The anastomosis is formed by the anterior ethmoidal artery the sphenopalatine artery the greater palatine artery and the superior labial artery. . Woodruff's area - venous plexus near the posterior end of the inferior turbinate. . in young people (below 35 years old) bleeding is usually from a small area. From middle age onwards the typical bleeding site moves posteriorly. Causes for epistaxis It may be either due to local or systemic diseases. Local causes are: Trauma - accidental (external trauma to the nose), intentional (repeated nose picking), surgical trauma (iatrogenic), foreign body in the nose. Nose infections - specially Atrophic Rhinitis Physiological epistaxis: Violent exertion or excitement like coughing, snooring, straining and blowing of the nose; longstanding on extremes of cold and heat - common schoolchildren. Tumours or malignancy of the nose and paranasal sinuses. Systemic causes are: Hypertension - in older people bleeding is often associated with degenerative arterial disease and hypertension. Leukaemia - childhood epistaxis is a symptom of leukaemia, vitamin K - deficiency. Many nose bleeds are idiopathy. Complications Hypovolumic shock - the elderly are particularly prone to suffering from shock which may be fatal, Anaemia; Nose Ulcers are other complications. Management Try to maintain the patient's general condition. In majority of cases, the bleeding is minor and stops spontaneously. When a patient is seen during bleed, initially firm uninterrupted pressure of the nostrils between finger and thumb for at least 10 minutes, possibly with an ice pack over the bridge of the nose. Once the bleeding is controlled, the nose is examined and the site located. If there is severe or continuous bleeding, patient may get shocks. If there are signs of a shock (pallor, cold peripheries, faints, pulse increase and hypertension), they should be hospitalised and ensure the airway remain clear. |
|
News | Business | Features
| Editorial | Security Produced by Lake House |

 Q: Dengue is often mistaken for an ordinary flu until it is too late.
How does one recognise the symptoms of this disease at the onset?
Q: Dengue is often mistaken for an ordinary flu until it is too late.
How does one recognise the symptoms of this disease at the onset?




