|

New National Institute for Nephrology opens at Maligawatte
by Nilma DOLE
 |
|
Dr. Alan Ludowyke
Pix by Chinthaka Kumarasinghe. |
Kidney problems are increasingly common in society today and with
this in mind, President Mahinda Rajapaksa decided that it was high time
to commission the National Institute for Nephrology, Dialysis &
Transplantation at Maligawatte, Colombo. Sudden outbreaks of Chronic
Renal Disease (CRD) have been rampant in the Uva, Central and North
Central Provinces in Sri Lanka.
Speaking to the Sunday Observer on the Nephrology Institute Dr. Alan
Ludowyke, the Medical Officer in charge of the Institute, said, "We need
time to have a proper system in place. Right after the President opened
the Institute, many patients came from far-flung parts of the country to
get themselves admitted but we still need to get the necessary equipment
and resources to fully-equip the Institute because a comprehensive
health service has to be provided to all patients. Also, we only get
referrals from the Dialysis Unit at the Colombo General Hospital from a
consultant and then admit them to the Institute." It is estimated that
there are about 1000 patients who need advanced treatment such as
dialysis and kidney transplant for their renal complications in Sri
Lanka, but only about 250 seek treatment at tertiary care hospitals.
Most of them perish before they even reach the hospital which is
unfortunate.
At the moment, the Colombo National Hospital provides dialysis for
kidney patients (who don't get a transplant) through the machine about
once a week when the requirement is actually thrice a week. "It is too
expensive for the Hospital to give kidney patients dialysis thrice a
week free of charge, since we cater to the poor strata of society", said
Consultant Nephrologist of the Dialysis Unit in the National Hospital,
Dr. A. L. M. Nazar. He said "We could cater to a maximum capacity of 29
but we have only 10 machines to meet the demand." As one of the senior
consultants to the Maligawatte Kidney Institute, Dr. Nazar said the New
Institute is a 100% government funded project but there has to be public
and private donations if it is to function successfully.
 |
|
Patients undergoing
dialysis treatment |
"We are happy that the government together with the University of
Colombo launched the new state-of-the-art kidney facility, but there are
small aspects that need to be taken into consideration," said Dr.
Ludowyke.
He said that there is a sewerage problem that needs to be dealt with
by the Colombo Municipal Council as the Institute is prone to flooding.
"In addition to this, the R. Premadasa District Hospital in Maligawatte
nearby also gets flooded causing more harm than good" said the doctor.
The canal nearby flows with dirty water and the water-pipe line that
runs through the Maligawatte township doesn't pump sufficient water for
the District Hospital, the Maligawatte Kidney Institute and the little
commercial and residential settlements along the main road.
Yet, this Institute was opened in a bid to invite qualified doctors
and professionals abroad to come back to the country to help the needy
patients. "Even though we have a team of 9 nurses, some junior nurses
and three temporary consultant nephrologists, we need additional hands
to help steer the Institute in the right direction. So we welcome
trainee doctors to specialize in this area and invite Sri Lankan medical
experts abroad to help in this sector", said the doctor.
Once completed, the National Institute for Nephrology, Dialysis &
Transplantation will be complete with 111 beds providing such facilities
as kidney disease diagnosis, dialysis and transplant surgery. According
to the sources, the total cost of the project was Rs. 450 Million, the
cost of the building component of the project being Rs. 403 million and
the equipment purchased so far amounted to nearly Rs. 40 million.
|

Head Nurse Matron Malithi Rathnagoda of the Dialysis Unit |
"In the initial phase, this institute will provide Nephrology
services through an Out-patients' Department, in-ward facilities of 60
beds in both the Nephrology ward and the Dialysis Unit" he said.
He explained "In the first phase, the Dialysis Unit will commence
functioning with 10 machines, with a total capacity for 24 machines in
the future. Transplantation services and ward facilities will commence
subsequently as the necessary equipment and staff becomes available".
He said the Institute is more than just a haven for kidney patients,
budding doctors who want to specialise in nephrology will have the
opportunity to obtain hands-on practical experience as it will be
developed into a research and training Institute. "The Junior training
staff at the Institute can always come back once they graduate to work
with us because the experience is valuable", said the doctor. "It is an
Institute for educational training in renal and transplant specialties
providing research and further development which will act as the apex
body in advising the Ministry on development of this sector. Hence, it
will develop a comprehensive database to determine epidemiology of
related diseases in order to assist in long term national planning to
develop services and be a link Institute with affiliations to
professional organizations, consumer groups and funding organizations",
Dr. Ludowyke said.
Explaining further he said that for a number of years, the
President's Fund has been helping individual patients with the high
expense that dialysis and transplant treatment entails. To ensure easy
access to quality and modern healthcare services for all with an
emphasis on the needs of the lower income groups and those most
vulnerable in society is the main focus of the Mahinda Chinthana and the
outcome is the Maligawatte Kidney project. Consultant Vascular and
Transplant Surgeon, Kidney Institute, Dr. S. D. Rajamantri said, "This
project was initiated in 1999 but the work stopped at foundation level
until 2004 when the building was redesigned to suit the modern needs.
Under the present administration, work proceeded on schedule and the
building was completed in early 2009".
He said that it is a timely event that this building has been
commissioned as the number of new cases of renal failure seems to be
increasing steadily. There is a conspicuous lack of research in this
area in the past, and they still do not have exact figures relating to
incidence, demographic distribution or the causative factors in kidney
disease in Sri Lanka. "I feel at least now the universities should look
into this aspect. The Minister of Healthcare & Nutrition has initiated a
project along with the World Health Organisation (WHO) to isolate the
causes for this epidemic in Sri Lanka, but I am not aware of the
details", said the doctor.
He said, "The NINDT is still equipped to function only for Dialysis,
which is only around 20% of its work capacity. All equipment purchases
to commission the rest of the building have been finalised, but we are
in need of funds to expedite this".
Once commissioned, this unit is designed to perform well over 200
kidney transplants annually, which is more than double the number that
is done in the whole country right now. "Transplantation is a cheaper
method for our country to manage these patients, and also affords a
longer survival and a much better quality of life to the patient",
stated Dr. Rajamantri.
In addition to this, he said, "We also hope to expand into cadaveric
kidney transplantations, to ease the shortage of live donors. This
hospital will also offer a round the clock service for cadaveric
transplantations and critical illnesses in transplanted patients."
Prevention is always better than cure. So make sure you drink at least a
litre of water (more is better) everyday to prevent kidney disease.
Influenza A(H1N1) kept at bay
by Nilma DOLE
 "Compared to other countries, Sri Lanka has managed to keep the
number of Novel Influenza A (H1N1) cases to a minimum", said Director of
the Epidemiology Unit, Dr. Paba Palihawadana. She said, "We have an
effective strategy in place to make sure that those inflicted with the
disease do not spread it and that the people are aware of it." "Compared to other countries, Sri Lanka has managed to keep the
number of Novel Influenza A (H1N1) cases to a minimum", said Director of
the Epidemiology Unit, Dr. Paba Palihawadana. She said, "We have an
effective strategy in place to make sure that those inflicted with the
disease do not spread it and that the people are aware of it."
Dr. Palihawadana said, "At the moment, Sri Lanka is working on
bringing down the recently developed H1N1 vaccinations to prevent the
high-risk groups from getting the disease." With the recent suspected
deaths across the island that included pregnant women too, it is now
imperative to safeguard the high-risk category against the disease.
Speaking to the Sunday Observer Consultant Epidemiologist Dr. Samitha
Ginige said, "Besides pregnant women, the high-risk groups include
children under 2 years, senior citizens and people with chronic ailments
including lung diseases and diabetic patients. It depends on the
patients' immune system and the stress suffered by the patient."
"Patients suffering from fever for more than 4 days with flu - like
symptoms should consult their nearest General Physician or a qualified
medical practioner to determine if they are really affected by H1N1",
said Dr. Paba Palihawadana. "Many think private medical treatment is
better than government hospitals but they should realise that the latter
is better equipped to deal with any outbreak with its experience. It is
also less expensive. The doctor said, "A doctor who suspects his
patients have H1N1 will send their samples to Medical Research Institute
for analysis".
The effective strategy maintained by the EPID unit is that they ask
people to be cautious and wary of themselves.
"The best advice I can give to parents is to be less harsh on their
children. Tuition classes and over-stress will weaken their immune
system. Make sure your child has a balanced diet. It is upto the parents
to look after their children very well," said the Dr. Palihawadana. "If
your child is prone to the flu then take precautions but don't overdo
it", she warned.
People shouldn't think that the Ministry is keeping H1N1 statistics
hidden but now that the flu has entered the country, we are not sure
about the accurate numbers as yet. It takes time to count the real H1N1
cases as and when the diagnosis is done and investigations concluded on
people who are suspected of having H1N1.
However, we should be careful because it is a fast-spreading disease
which can be cured easily", Dr. Ginige said.
"When using masks, it should be handled with care. It is better if
particularly the patients wear it to prevent from getting the flu", he
said. He added, "There is a special method of using masks prevent its
spread."
He stated that some people who are asymptomatic but have the virus
with them spread it.
"However, it is best for the ordinary individuals not to be scared of
getting the flu but eat a balanced diet, exercise, have a good immune
system and maintain good personal hygiene", said Dr. Ginige.
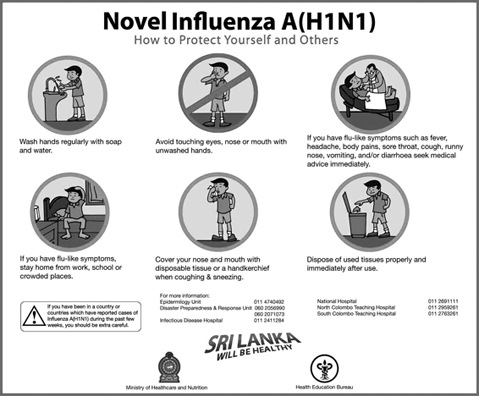
How to Avoid H1N1
1.Avoid public gathering places as much as possible. Infection is
likely to spread rapidly in places where there is a high concentration
of people.
2.Do not send infected children to school. Make sure they get
plenty of rest and wait at home until they have recovered fully.
3.Wash your hands properly with ordinary soap and water. It is
better to use a tissue paper but if you're using a handkerchief, make
sure you wash it and not use it to blow/wipe your nose.
4.Maintain strict personal hygiene.
5.Pregnant women, senior citizens, young children and those with
chronic ailments should be extra careful. If they have persistent
flu-like symptoms, immediately consult a doctor.
Obesity in childhood
by Dr. D. P. Atukorale
 There has been much publicity about health problems due to obesity in
adult life in the newspapers and medical journals. But there is less
appreciation of issues surrounding obesity in children and adolescents.
A large number of people believe that childhood obesity is just a
cosmetic problem and diagnosis of obesity in childhood is less robustly
performed than for adults. There has been much publicity about health problems due to obesity in
adult life in the newspapers and medical journals. But there is less
appreciation of issues surrounding obesity in children and adolescents.
A large number of people believe that childhood obesity is just a
cosmetic problem and diagnosis of obesity in childhood is less robustly
performed than for adults.
Many parents in Sri Lanka don't consult their paediatricians or
dietician when they have obese children and some Sri Lankans have the
misconception that obesity in childhood is a sign of good health and so
they never take these obese children to paediatricians for advice and
thus obese children in Sri Lanka don't get the appropriate treatment.
The rise in the prevalence of childhood obesity in U.K. has been
appropriately labelled as an epidemic and the adverse consequences of
childhood obesity are increasingly recognized (Armstrong J et al, Arch,
Dis, Chil. 2003:88:671-5; Reilly J. J. Dorsty AR, Lancet,
1999:354;1874-5.
It is common knowledge that childhood obesity persists into adult
life. Obesity in children is different from obesity in adults. The most
obvious difference is that children and adolescents need to grow during
puberty: adolescents will double their weight and increase their height
by 20 per cent. In adults, obesity is expressed as body mass index (BMI,
weight in kilograms divided by height in metres squared) In adults a BMI
of 26-30Kg/m2 is considered overweight, BMI of 30-40 is considered
obese, and BMI greater than 40 is considered morbid obesity. But in
children such a simple expression of obesity unrelated to age, sex or
ethnic background is not possible. In obese children over enthusiastic
management of obesity may result in restriction of dietary energy and
would compromise normal growth and development. Unlike treatment of
adult obesity, weight maintenance is often a suitable goal in childhood.
Clinical nutrition assessment in childhood and adolescence revolve
around energy (food) intake minus energy output (resting metabolic rate
plus activity). In contrast to adult life where energy balance should be
zero, children need a small continuing positive energy balance to
support normal growth. An excess continuing positive balance will lead
to excess stores of energy and thus obesity. It is not only fat which
accumulates but also excess of lean body mass. The sources of chronic
energy-positive balance leading to obesity are increased energy (food)
in take and reduced energy expenditure by either lack of physical
activity or an increase in sedentary behaviour. The simple energy
balance equation is poorly understood by some of the parents of these
obese children who often believe that their children have metabolic
problems.
Prevalence of obesity
In U.K. adult epidemic of obesity began in late 1970's and childhood
obesity probably started 10 years later. "The Health Survey for England"
showed that in 1991 the prevalence of obesity (defind as BMI 95th
centile for age and sex) was nearly 10 per cent at 6 years of age, 12
per cent at 10 years of age and 17 per cent at 15 years of age. It was
shown that in Scotland that in 1999, 9 per cent of children in the first
year of primary school were obese and this had reached 16 per cent at
the age of 15 years. It can therefore be truly stated that obesity is
the most common disorder of childhood and adolescence. (Amstrong et al,
Arch. Dis. Child,2003.88.671-5). There is a definite link with
socio-economic deprivation and obesity in Scotland. The issue of whether
breast feeding is protective against later development of obesity
remains a controversial issue.
Childhood obesity is becoming a more and more common in the higher
socioeconomic groups especially in the urban areas of Sri Lanka. As far
as I am aware, there are no statistics regarding prevalence of obesity
in childhood and adolescence in Sri Lanka. One cause of childhood
obesity is due to more food eaten away from home. Another cause of
childhood obesity is lack of physical activity.
Consequences of obesity in childhood
Does childhood obesity matter? The most common side-effect of
childhood obesity is psychological morbidity. In obese children there is
an increase in a cluster of cardiovascular risk factors such as
hyperlipidaemia, high blood pressure and abnormalities in left
ventricular mass, hyperinsulinaemia and prevalence of type II diabetes.
There is a link between childhood obesity and bronchial asthma and rarer
complications are orthopaedic problems and development of fatty liver.
The consequences of childhood obesity for adult life are persistence of
obesity, significant increase in cardiovascular risk factors,
socio-economic effects and long term morbidity and mortality.
Prevention and Treatment of Childhood Obesity
There is no evidence at all that drug therapy or surgery is of any
help in these obese children. There should be reduction in sedentary
behaviour, increase in lifestyle physical activity dietary approach and
family involvement.
There is also evidence to show that childhood obesity is a social
problem rather than one that we can expect individual children and their
parents to solve. (Schwartz MB, Puhl R, Obesity Rev. 2003,4,57-7)
Reference: The Journal of Royal College of Physicians of Edinburgh, Vol.
34:8-10, 2004]. |
















")