|

Correct body weight, lifestyle changes prevent arthritis
By Carol Aloysius
While the symptoms of arthritis, are usually visible when one reaches
middle age and above, their debilitating effects take place much
earlier, the foundation often being laid in early childhood. Arthritis,
although a common condition, is not curable once a person is afflicted
with it. Treating arthritis patients especially in a welfare nation such
as ours, costs millions of rupees for the state. Preventing this disease
is not costly or complicated, as it needs mostly a change in one’s life
style, which will minimise the effect of arthritis to a large extent,
says a leading Rheumotologist.
 Consultant Rheumotologist National Hospital, Dr Lalith Wijayaratne
gives us an insight into the disease and the rehabilitative services
available for arthritis patients in state hospitals. Consultant Rheumotologist National Hospital, Dr Lalith Wijayaratne
gives us an insight into the disease and the rehabilitative services
available for arthritis patients in state hospitals.
Excerpts…
Q. What are the objectives and significance worldwide and in
Sri Lanka of Arthritis Day which fell yesterday?
A. The aims of World Arthritis Day are:
• To raise awareness of arthritis in all its forms among the medical
community, among people with arthritis and among the general public.
• To influence public policy by making decision-makers aware of the
burden of arthritis and the steps which can be taken to ease it.
• To ensure all people with arthritis are aware of the facilities
available to them. Observing this Day worldwide, is significant due
programs that educate people how they can prevent this disease with
simple interventions such as changing their lifestyles.
Q. Is Arthritis mostly a disease of the elderly? Can a young
person also get it?
A. It is a disease of middle age and elderly persons. But
children too can get arthritis.
Q. What ages do you consider are the high risk groups?
A. From 20 to 40 years
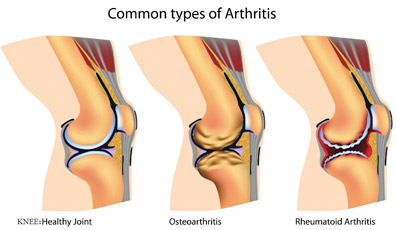
Q. Are there different types of arthritis? Is osteoarthritis
and arthritis the same?
A. Arthritis occurs as a result of inflammation (swelling,
warmth and redness - soreness) of the delicate structures within the
joint.
The common types of arthritis seen in Sri Lanka include: Rheumatoid
arthritis, Psoriatic arthritis, Ankylosing spondylitis, Reactive
arthritis, Gout and Systemic lupus erythematous.
Osteoarthritis is different to arthritis. The underlying problem with
osteoarthritis is wear and tear or degeneration of the cartilage which
gives a cushioning effect to the joints
Q. Of all these forms, what form of arthritis is most commonly
found in Sri Lanka?
A. Osteoarthritis
Q. Arthritis is said to be a rheumatic and musculoskeletal
disease. Which part of the body dues it affect specifically? The joints?
Neck? Knees? Knuckles?
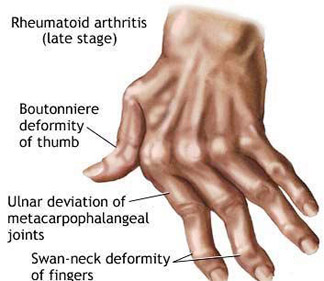
A. Rheumatoid arthritis affects the knuckles, hands, feet,
ankles and wrists. Osteoarthritis affects the weight bearing and the
frequently moving joints such as knees, hips, lower spine, neck and the
hands. Ankylosing spondylitis affects the joints of the spine
Gout affects joints of the feet, ankles and knees
Q. What other organs are affected by arthritis?
A. Heart, lungs, skin, blood cells, blood vessels, nerves,
Q. What are the causes? Food ? Lifestyles? Genes?
A. Lifestyles and genes
Q. What are the symptoms of arthritis?
A. Pain, swelling and stiffness of joints. In extreme and long
standing patients – excess of fluid within the joints and joint
deformities.
Q. Is numbness of the toes and feet a symptom?
A. This is not a direct effect of arthritis, although some
arthritis patients do feel numbness in their feet due to the involvement
of the peripheral nerves.
Q. If pain and stiffness are symptoms, how can they be
differentiated from the kind of pain and stiffness one experiences when
sitting too long at a computer?
A. Stiffness of arthritis lasts for more than 30 minutes.
Usually accompanied with symptoms of fatigue, tiredness, loss of
appetite, night sweats and feeling low. The pain and stiffness that one
experiences from arthritis can disturb their sleep in the early hours in
the morning. They wake up with stiffness.
 Q. Can early detection prevent or minimise arthritis? Q. Can early detection prevent or minimise arthritis?
A. Definitely YES.
Q. Can the condition be reversed with medication?
A. Not reversed. But it can arrest the progress of the
disease.
Q. Can diet help? If so what kind of food should one eat?
A. Avoiding food which can put on weight (e.g. food with a
high saturated fat content), can minimise an excessive load on the joint
which can make the arthritis joint to get more damaged.
Q. How early in life should one prepare to prevent developing
arthritis?
A. From a very young age. By doing regular exercises,
preventing putting on too much of weight, training the mind not to get
over active in stressful situations.
Q. Once you get arthritis, can you cure it? Or simply have to
live with it ?
A. We can CONTROL arthritis, which will stop the progression
of the disease.
This is very much similar to the control of blood sugar and blood
pressure in patients with diabetes and high blood pressure. Therefore,
the emphasis is on early recognition and continued treatment.
Q. What happens when the disease advances? Is surgery the only
answer?
A. There is medical rehabilitation where the allied health
professionals such as physiotherapists, and occupational therapists join
hands with the doctors and implement a comprehensive rehabilitation
program mainly through exercises and various games which will help to
control the disease to a certain extent. When both drugs and
rehabilitation treatment fails the patient is referred for surgery.
Q. Are there different types of drugs to treat it? Are they
available here?
A. Yes.
1. Analgesics – to relieve pain.
2. Non-steroidal Anti Inflammatory drugs ( NSAIDs) which will reduce
the degree of inflammation and make the joints less painful and less
stiff.
3. Steroids.
4. Disease Modifying Anti Rheumatic agents( DMARDs) which will act on
the underlying immunological derangement which in turn will help to
control the disease.
5. Biologics - Very special drugs which will target important cells
and certain molecule which play an important role in propagating the
arthritis thereby controlling the disease.
Q. What exercises do you recommend that have the least stress
on the affected part?
A. The type of exercise the arthritis patient needs will
strongly depend on the type of joints involved, the degree of the joint
damage and on the patient’s overall health. Ideally a doctor should
guide the patient on exercises. But as a rough rule, whatever physical
activity does not cause pain should be practised daily on a regular
basis.
Those patients whose hips, knees, ankles and feet are not much
affected, a regular walk for about 15 to 20 minutes will help them.
Q. Can applying heat and cold help to reduce the pain?
A. Yes certainly. But if there is fluid in the joint or severe
soreness indicated by redness and warmth we discourage using heat. In
such instances ice will help more.
Q. Are there recent breakthroughs in treatment worldwide? Are
they available in Sri Lanka too?
A. Yes. Today we target our treatment to achieve disease
control or low disease activity. There are well tested and well defined
end-points for the doctors to identify when patients achieve the target.
Most of us follow this concept of treat to target when we are
treating all our patients with arthritis. There is this special group of
drugs what we call as biologics (Biological DMARDs) which help to
control the disease activity in patients whose disease is quite
aggressive not responding to standard therapy. We do have Biological
drugs in Sri Lanka.
Q. Does the National Hospital have a special unit to treat
arthritis patients and provide them services they need under one roof?
What does it do?
A. The National Hospital and also all the Teaching hospitals
and some General Hospitals in Sri Lanka have special units to cater to
the needs of patients with arthritis. These units are called
“Rheumatology and medical Rehabilitation Units”.
A fully qualified (Board Certified) Consultant Rheumatologist is in
charge of this unit. Nurses, physiotherapists and occupational
therapists dedicated to care for patients with arthritis, also staffs
these units.
Patients need to carry a referral letter from any doctor to be
registered in these clinics.
The arthritis patients are treated with drugs as well as
rehabilitation treatment in these units.
Drugs are issued for one month. All the patients are regularly
followed up in these clinics and they are treated to achieve a disease
control. Colombo, Ragama, Colombo South, Galle, Matara, Jaffna, Kandy,
Nuwara-Eliya, Gampaha, Negombo, Kurunegala, Ratnapura and Kalutara are
some hospitals in the State sector which have a fully functioning
Rheumatology and Rehabilitation unit.
Q. You have recently started a peer group for arthritis
patients. What is its objective?
A. To work together as a team to get their Rights. These
include: The Right to get correct treatment. Right to be independent in
their day to day activities.
Right to be part of the society. To help the clinicians to improve
the services delivered to patients with arthritis by joining them to
make representations to the government authorities.
Educate the general public on arthritis and its consequences.
To educate and counsel patients on whom arthritis has been newly
diagnosed.
Q. Does having NCDs such as diabetes, hypertension and
cholesterol lead to and aggravate arthritis?
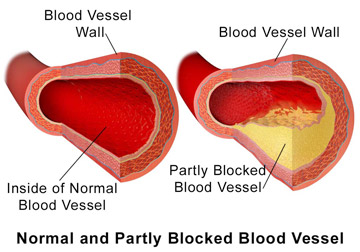
A. No. But as Arthritis is a known major risk factor for the
development of heart attacks and strokes these NCD conditions in an
arthritis patient can make the arthritis patient more vulnerable.
Q. Your message to the public?
A. Arthritis is a common condition. The
impact of arthritis can be made minimal by taking treatment as early as
possible, preferably within the first three months after developing the
first symptom. Maintaining correct lifestyles will minimise the effect
of arthritis to a greater extent.
Q. Do you have any ‘ golden’ rules for
preventing arthritis ?
A. Maintain ideal body weight
Do regular exercises
Food in moderation
Tame and train your mind so that it does not
get over-active in stressful situations.
Is food addiction a step closer to formal diagnostic status?
Food addiction is not yet recognised as a mental disorder but certain
obese individuals clearly display addictive-like behaviour towards food.
To achieve a formal diagnostic status, ‘food addiction’ requires a
stronger evidence base to support the claim that certain ingredients
have addictive properties identical to addictive drugs of abuse. This
topic is up for debate in the session, ‘Binge eating obesity is a food
addiction'.
 This year's fifth edition of the DSM (Diagnostic and Statistical
Manual of Mental Disorders) recognises ‘binge eating disorder’ (BED) as
distinct from Anorexia nervosa and Bulimia nervosa, but it remains
debatable whether BED is underpinned by an addiction disorder and should
be prevented and treated like other addictive disorders. This year's fifth edition of the DSM (Diagnostic and Statistical
Manual of Mental Disorders) recognises ‘binge eating disorder’ (BED) as
distinct from Anorexia nervosa and Bulimia nervosa, but it remains
debatable whether BED is underpinned by an addiction disorder and should
be prevented and treated like other addictive disorders.
The new category ‘Substance related and addictive disorders’ in DSM-5
combines the DSM-IV categories of substance abuse and substance
dependence into a single disorder measured on a continuum from mild to
severe.
Importantly, the term ‘dependence’ is not used any more in DSM-5,
because most people link dependence with addiction when, in fact,
dependence can be a normal body response to a substance.
Speaking at the 26th ECNP Congress Professor Suzanne Dickson,
neuroscientist from the Institute of Neuroscience and Physiology,
Sahlgrenska Academy at the University of Gothenburg, Sweden said, “the
introduction of ‘addictive disorders’ allows classification of
behavioural addiction for the first time, for example with pathological
gambling, but this does not apply to food addiction.
Although there might be neurobiological and clinical overlaps between
‘addictive-like’ overeating and substance related and addictive
disorders, a major difference is that is that food consumption, unlike
alcohol, cocaine, or gambling or internet gaming behaviour, is necessary
for survival.”
“A subgroup of obese patients indeed show ‘addictive-like’ properties
with regard to overeating, such as loss of control,” continued Prof
Dickson, “but this does not automatically mean they are addicted.”
According to some studies, at least 10-15 percent of obese
individuals suffer from BED. However, BED also occurs in people that are
normal weight.
The term ‘food addiction’ has been coined by the popular press and by
many sufferers as a reasonable explanation for their predicament.
Studies exploring the brains of obese patients that score highly for
food addiction on the Yale
Food Addiction Scale show that certain areas known to be involved in
reward and addiction have an altered response to both images of
appetising foods and even to the taste of food.
However, more evidence is needed to support inclusion of food
addiction as a diagnostic category.
Prof Dickson said: “This evidence itself is insufficient to support
the idea that food addiction is a mental disorder.
- Medicalxpress
Healthcare providers should target unhealthy lifestyles
Healthcare providers should treat unhealthy behaviour as aggressively
as they treat high blood pressure, cholesterol and other heart disease
risk factors, according to an advisory published in Circulation .
 “We're talking about a paradigm shift from only treating biomarkers -
physical indicators of a person's risk for heart disease - to helping
people change unhealthy behaviour, such as smoking, unhealthy body
weight, poor diet quality and lack of physical activity,” said Bonnie
Spring, lead author of the statement and a professor of preventive
medicine and psychiatry and behavioural sciences at North-western
University in Chicago. “We're talking about a paradigm shift from only treating biomarkers -
physical indicators of a person's risk for heart disease - to helping
people change unhealthy behaviour, such as smoking, unhealthy body
weight, poor diet quality and lack of physical activity,” said Bonnie
Spring, lead author of the statement and a professor of preventive
medicine and psychiatry and behavioural sciences at North-western
University in Chicago.
“We already treat physical risk factors that can be measured through
a blood sample or a blood pressure reading in a doctor's office, yet
people put their health at risk through their behaviour.
We can't measure the results of these behaviour in their bodies yet.”
Among the statement's recommendations, healthcare providers should
create “inter-professional practices” to connect patients with behaviour
change specialists such as dietitians or psychologists and implement the
five A's when caring for patients:
- Assess a patient's risk behaviour for heart disease.
- Advise change, such as weight loss or exercise.
- Agree on an action plan.
- Assist with treatment.
- Arrange for follow-up care.
For inter-professional practices to work, reimbursement policies must
be revised, Spring said.
Under an effective healthcare system, professionals can work with
patients and draw on community and technology resources to provide
intensive behaviour interventions. “This isn't a problem that can be
solved alone by the patient or the doctor who is strapped for time,”
Spring said. “We need to break out of our silos and get ahead of the
curve in prevention.” She said to achieve the American Heart
Association's 2020 impact goals - to improve the cardiovascular health
of all Americans by 20 percent while reducing deaths from cardiovascular
diseases and stroke by 20 percent-we must make preventing cardiovascular
diseases a priority.
- MNT
|












")
