|

Preventing diabetes - key to safe motherhood
By Carol Aloysius
Diabetes is on a sharp upward curve in Sri Lanka, with one in 10 over
20 years and one in four adults over 40 years having type 2 diabetes.
While all those afflicted by the disease are at high risk of
developing other non communicable diseases such as hypertension and
cardiovascular disease, women are more at risk than generally thought.
Diabetes in a pregnant woman affects both the mother’s health and that
of her unborn child. The key to preventing it is by adopting healthy
lifestyles starting at an early age leading to healthy mothers.
Professor of Reproductive medicine, Dept. of Obstetrics and
Gynaecology, Faculty of Medicine, University of Colombo and Hony.
Consultant physician and endocrinologist De Soyza Maternity Hospital, Dr
CHANDRIKA WIJEYERATNE talks to the Sunday Observer on how diabetes can
be prevented and why women play a key role in ensuring a healthy nation.
 Excerpts Excerpts
Q. Diabetes is one of the commonest non communicable diseases
in the world and in Sri Lanka. Your comments?
A. Diabetes has shown an exponential increase in its
occurrence in the past two decades. Sri Lanka, although a lower middle
income country has experienced similar changes in the increase of
diabetes mellitus and risk factors for cardiovascular disease very
similar to high income countries. One in ten of Sri Lankans over the age
of 20 years and one in four of adults over the age of 40 years have type
2 diabetes.
Q. How do you describe diabetes? What causes it?
A. The commoner variety - type 2 diabetes mellitus is a
situation where your insulin hormone produced by the pancreas cannot act
on cells to help glucose to enter into the cell for it to function
properly. This is due to a resistance of the insulin receptors.
The cause of this resistance is excess body fat or adipose tissue.
The resulting high blood glucose affects the function of blood
vessels throughout the body. The larger blood vessels tend to get
blocked by atheroma (fat deposits) that can cause heart attacks, strokes
and poor circulation to the feet.
Affection of small vessel function can cause diabetic kidney failure,
eye disease, erectile dysfunction and nerve dysfunction.
However, the majority of people with type 2 diabetes do not
experience any symptoms, until the organ function gets affected. It is
estimated that one third of Sri Lankans with diabetes are unaware of
this affection.
Q. Can it be inherited?
A. Diabetes does run in families. A recent study in the urban
setting showed that one in ten households have diabetes. The great
majority of these are due to unhealthy lifestyles.
Q. What are the different types of diabetes?
A. The three major types
1) Type 1 diabetes - which is a lack of production of insulin by the
pancreas that causes extreme thirst, excess passage of urine and a risk
of diabetic coma (ketoacidosis.)
2) Type 2 - is the adult onset type due to insulin resistance and
the commonest variety.
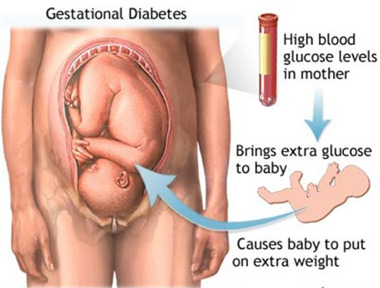
3) Gestational diabetes - is diabetes that occurs during pregnancy,
caused by the major hormone changes that unmasks diabetes.
Q. Who are most at risk? Men? Women? Youth? Elderly?
A. An increasing number of women are reported to develop type
2 diabetes due to unhealthy lifestyles. In the great majority, this can
be prevented if young individuals at risk adopt healthy lifestyles In
the very elderly, when the organs shrink they can develop a relative
lack of insulin.
|
Five healthy
tips for pregnant women
1. Sleep at least eight hours a day..
2. Prevent constipation by eating whole grains, cereals, raw fruits,
vegetables, and drink at least 8 glasses of water a day.
3. Don’t take laxatives drugs, enema, medicines or home remedies unless
your doctor recommends them.
4. Milk gives you extra protection, calcium and other nutrients you need
when pregnant.
5. Tea, coffee, cocoa and chocolates as well as fizzy drinks have
caffeine which is harmful to the unborn child.
- US Dept of Public Health
|
Q. Which age group is highest at risk in Sri Lanka? Why?
A. Those beyond the age of 40 - midlife - are the greatest
numbers detected each year. The reason is less organ reserve with
greatest risk of insulin resistance due to increased fat tissue in the
body.
Q. How do you diagnose diabetes?
A. Blood glucose testing is the best method of detection.
Following an overnight fast of 8-12 hours if your fasting blood glucose
is less than 100 mg/dl you are unlikely to have diabetes.
If your FBG is greater than 126 mg/dl on two occasions this confirms
that you have diabetes. Those with FBG between 100 and 125 have impaired
fasting glucose (pre-diabetes) that can also be prevented from turning
into full blown diabetes by a change from unhealthy to healthy
lifestyle. The gold standard test is the 75g oral glucose tolerance test
(OGTT) which can confirm pre-diabetes and diabetes.
Q. Is diabetes reversible?
A. It can be controlled and kept in check. There is no
permanent cure for type 2 diabetes.
Diabetes in mothers
Q. Today, we see an increasing number of young women including
young mothers being diagnosed with diabetes, some of them for the first
time when they come to a maternity clinic. Your comments?
A. The greater majority of young women develop diabetes during
pregnancy. This is called gestational diabetes (GDM) and afflicts about
1 in 10 mothers-to-be.
They develop GDM because of a greater potential to develop diabetes
later in life due to excess body fat and family risks.
Pregnancy unmasks this risk due to the major hormonal changes that
arise from the growing placenta. These hormones act usually arise around
the 5th of pregnancy and after by acting against the mother’s insulin
and thereby the pregnant mum develops high blood sugar during pregnancy.
However, due to their unhealthy lifestyles, young women who have
developed diabetes may be unaware of this when they conceive.
This is actually pre-pregnant diabetes and has worse complications
due to the high blood sugar being present from conception itself.
High blood glucose in the mother in the first three months of
pregnancy can cause abnormalities in the developing foetus that can be
prevented by recognising the woman’s diabetes and controlling this to
normal blood glucose targets
Q. Is gestational diabetes reversible? Will it disappear after
a while?
A. Gestational diabetes will get worse during the pregnancy if
undetected and uncontrolled.
Then the high maternal blood glucose can cause ill effects on the
unborn baby with a higher risk of foetal death or complications around
birth. Additionally the mother can develop high blood pressure.
However, with the delivery of the placenta, the hormones that rake up
the mother’s blood glucose subside in her system, and the GDM can revert
back to normal.
But if the mother does not lose weight and adopt a healthy lifestyle
she is at greater risk of developing GDM in a subsequent pregnancy or
even develops type 2 diabetes even without being pregnant.
Q. How is gestational diabetes managed?
A. We recommend a healthy meal plan and physical activity and
monitor the blood glucose.
The mother needs to have normal blood glucose appropriate for
pregnancy throughout the day and throughout her pregnancy. The blood
glucose values are much lower than those stated earlier.
The reason for this is there is a proportion of blood glucose that
passes on to the foetus for which we need to make an allowance.
Therefore we maintain a pregnant woman’s blood glucose at less than
90 mg/ dl before a meal and less than 120 mg/dl 2 hours after a meal.
Q. Is insulin safe for pregnant mothers?
A. Insulin is very safe for mum and baby. However, the tablet
metformin is being increasingly used for those with major insulin
resistance.
Q. What are the health complications if the mother is
untreated for 1) the mother 2) the baby?
A. The mother is at greater risk of developing high blood
pressure in pregnancy that has its own set of major complications.
This can be prevented to quite an extent by early detection and good
control of blood sugars.
Poorly controlled diabetes means the unborn baby gets excess glucose
from the mother that is toxic to baby. The baby becomes unhealthy with
excess body fat or in some cases poor foetal growth that can place the
foetus at great risk of death or complications.
Q. Statistics on the number of diabetic mothers in Sri Lanka?
A. Approximately 400,000 women get pregnant per year and 10
percent of them have diabetes - that is approximately 40,000
Q. Have the numbers of diabetic mothers treated by you
declined or gone up in the past 10 years? Why?
A. No it keeps increasing at a younger age. Preventing
diabetes starts from childhood and adolescence.
It requires a life cycle approach. Mothers can prevent getting
diabetes by adopting healthy lifestyles and screening themselves prior
to conception.
Q. At what age is a girl most vulnerable to developing
diabetes?
A. Puberty makes one vulnerable to insulin resistance due to
the excess fat deposition.
Thereafter pregnancy is the next phase when insulin resistance can
set in with the growth of the placenta.
Q. Can a baby develop diabetes in the womb if her mother is
diabetic, or eats too many sugary foods while pregnant?
A. The excess sugar that is passed on to the unborn child does
not cause diabetes but causes excess body fat. Such girls and boys have
a greater risk of obesity from a very young age.
Q. Has new research on diabetes especially in relation to
pregnant mothers young mothers provided a breakthrough in treating them?
A. Prevention is the best form of treatment through healthy
lifestyles - diet and physical activity
Q. I understand that the Sri Lanka Medical Association is
setting up a special service to save mothers from developing diabetes
and other non communicable illnesses. Your comments?
A. The SLMA has established a large project to assist the
Ministry of Health named Nirogi Lanka with funding from the World
Diabetes Foundation.
In its second phase, we have introduced the concept of Nirogi Maatha
(healthy mother).
The Ministry of Health has a super track record of attaining
excellent maternal and child health services by a low cost equitable
field service that ensures the great majority of pregnant women are
registered early in pregnancy for ante-natal care and also follow up the
babies.
The Family Health Bureau is the focal point for coordinating this
valuable service. We work along with Family Health Bureau which
coordinates this service, to ensure that every pregnant woman
is screened by blood sugar testing for GDM and follows an appropriate
diet and physical activity from pre-conception to post pregnancy and
lactation.
Mothers with GDM need long term support to prevent developing future
diabetes. Our theme is ‘healthy mothers result in healthy families and
societies’.
Q. Advice to women in general and pregnant woman particularly,
on preventing, controlling and treating diabetes?
A. Adopt healthy lifestyles. View pregnancy as a normal but
valuable phase of your life.
Unhealthy diet is calorie dense with excess starch, sugars, fats and
excess salt– that often come from fast foods and drinks. Brisk exercise
such as walking at least for 30 minutes a day 5 days of the week, can
keep you free from most non communicable diseases including diabetes.
Taking pre-pregnancy folic acid and ensuring you have taken your
rubella vaccine is also your responsibility.
Finally, plan your pregnancy and your family, to create a healthy
nation.
Overcoming kidney disease vital for a healthy nation
by Dr A.T.W. Guneratne
It is a well known fact that there is a significant increase in the
incidence of cancer, liver and kidney failure, allergic reactions,
nervous system disorders, and sterility. One common cause for this is
the toxic chemicals we are consuming with food and water.
Large scale vegetable growers use weed killers, insecticides,
fungicides and large amounts of chemical fertilisers to optimise their
crop. Some vegetable growers do not use insecticides to the vegetables
they consume, as they know that it is bad for their health.
The most insecticide sprayed vegetables are apparently the upcountry
grown. e.g. cabbage, leeks, tomatoes, beans etc.
There is no control in the use of insecticides; some farmers may not
know the consequences of consuming insecticide contaminated vegetables.
Agro chemicals should not be sprayed at least two weeks before
harvesting. Sometimes the concentration of agro chemicals used exceeds
the recommended levels as given in the instruction leaflet.
Some insecticides, fungicides and chemical fertilisers have toxic
heavy metals as impurities e.g. Arsenic, cadmium, lead. The authorities
concerned should analyse all agrochemicals used in agriculture and ban
the import of toxic ones. Some have already been banned. If vegetables
are kept soaked in water for 1-2 hours and washed well before cooking
most of the surface agro chemicals will be removed.
Ideally it is best to grow your own vegetables and green leaves at
home. Lack of space may be a limiting factor, but if you are really keen
you could grow vegetables and green leaves in pots or large polythene
bags. I have seen how vegetables are grown on roof tops.
 While
flowers are being grown some space may be reserved for vegetables and
green leaves. Compost which could be produced in your home or bought
from a fertiliser store and cow dung available in bags in fertiliser
stores are all what is needed with sun light and water to start your
vegetable garden. You will be very happy to see your home garden thrive
and in addition to have poison free vegetables and green leaves. In
addition you will save on the money spent on vegetables. While
flowers are being grown some space may be reserved for vegetables and
green leaves. Compost which could be produced in your home or bought
from a fertiliser store and cow dung available in bags in fertiliser
stores are all what is needed with sun light and water to start your
vegetable garden. You will be very happy to see your home garden thrive
and in addition to have poison free vegetables and green leaves. In
addition you will save on the money spent on vegetables.
In foreign countries there is a good demand for organic food. Even in
Sri Lanka there are a few organic food outlets. Organic vegetables are
produced without chemical fertiliser and agrochemicals, but they are
expensive as yields are less, but there is a growing demand. Organic tea
is also available in Sri Lanka but is mainly exported.
Fruits
In large scale commercial fruit cultivations, agrochemicals and
artificial fertilisers are used similar to large scale vegetable
cultivations. Fruit sellers use chemicals to enhance fruit ripening and
also to protect fruits from insects.
Frequent checking of fruit cultivations and testing for chemicals in
large fruit distributors, prohibiting the sale of toxic fruit ripening
chemicals and educating farmers and fruit distributors will reduce the
toxic chemicals in fruits.
If fruits could be bought from home gardens or you grow your own, it
will be the ideal solution.
Paddy cultivation
To increase yields paddy cultivators use agrochemicals, large amounts
of artificial manure and insecticides which are sprayed close to
harvesting. The rice we consume must be analysed to exclude toxic
chemicals. Imagine the plight we would be in if the rice we eat is
poisoning us.
Large amounts of weed killers and chemical fertilisers are used in
the tea estates; as such, tea has to be analysed for chemical toxicity.
In large poultry and dairy farms both in Sri Lanka and abroad vitamins,
antibiotics, nutritional supplements and hormones are given to enhance
the production of eggs and milk. Some of these enter eggs and milk which
could cause harmful effects on the consumers. The ideal would be to
obtain eggs ( gam biththara ) from small scale egg producers.
In some of the fast food outlets certain chemicals are added to
increase taste and smell. Some of them may cause allergy while others
may be carcinogenic. Some small food outlets wrap the food in
newspapers. The printing dye in newspapers are toxic to the human body,
food should never be wrapped in newspapers. There may be traces of toxic
chemicals in the food we eat and the water we drink, but the human body
could get rid of these if the intake is not excessive to overwhelm these
organs. With old age the function of these organs decreases, therefore
most organ failures occur in old age.
Could we stop using agrochemicals and artificial fertiliser in
agriculture and other food related industries? This is not possible as
the yields will drop and it will not be profitable to do agriculture. We
must encourage farmers to use more compost manure, reduce artificial
manure, control and reduce agrochemical use, produce high yielding
varieties of paddy, vegetables, tea etc. Already a number of high
yielding verities are being used.
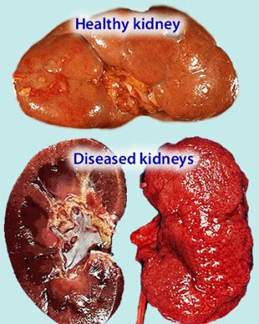
Chronic Kidney Disease (CKD)
It well a known fact that a large number of farmers in the North
Central Province have died of CKD and that there are large numbers
having this disease. It has been observed that this disease is gradually
spreading to the adjacent areas. According to estimates the population
at risk is about 2.8 million. Though a specific cause is not known, it
is believed to be multi-factorial in origin. The water in most of the
affected areas is polluted with agrochemicals and toxic heavy metals,
arsenic, cadmium, lead and fluoride. There is no cure for chronic renal
failure, dialysis is a temporary mode of treatment, renal transplant s
are the only possible long term treatment, but only a limited number of
transplants could be done and are very expensive. The only solution is
to prevent the development of CKD.
Prevention of CKD
CKD is due to the consumption of polluted water and food.
Agrochemicals and artificial fertiliser in excessive amounts contaminate
wells, streams rivers, irrigation tanks and also the soil. The farmers
must be educated regarding the problem faced by them. All sources of
drinking water must be checked to find out whether they are fit for
drinking. A centrally purified pipe borne water supply is the ideal
which the government has started, but it will take a long time and lot
of money to do so. Rain water harvesting is a practical, relatively
inexpensive way to obtain clean drinking water.
People in the affected areas should be encouraged and helped to
construct the tanks to collect rain water. Polluted water could be
purified by a method known as reverse osmosis, which is a relatively
cheap way of providing clean water from polluted brackish water.
People in the north central province and adjacent areas should be
educated regarding the causation of CK and how to prevent it.
Foreign aid agencies, NGOs, and village level organisations such as
Sarvodaya should be mobilised as an emergency, as there is not much
time. If the present trend continues, in five to 10 years there may be a
shortage of farmers and our paddy cultivation will be adversely affected
and we may have to get down farmers from foreign countries to work our
fields.
The authorities must coordinate and mobilise all relevant ministries
and organisations and provide adequate funds to prevent a disaster in
the near future.
The writer is a
Consultant Paediatrician
|











")


