|

Gene-technology unveils new dengue strains
By Carol Aloysius
As dengue continues to spread with over 23,355 cases being reported
islandwide for the first seven months of the year, by the Epidemiology
Unit, concerned health officials are turning for help to genetic
technology scientists to enhance their surveillance tools and prepare
themselves to meet the challenges of future dengue epidemics in the
country.
|

Scientists at work at the Gene-technology Lab |
Scientists researching the virus at the Gene Research Institute (GRI)
at Kitulwatthe using genetic technology have recently discovered some
startling facts behind the dengue epidemic which peaked in 2009 which
could prove to be a breakthrough for better dengue surveillance in
future. These facts were presented in a research paper in 2011.
The Director/ Senior Research Scientist, Genetech Research Institute,
Dr Dharshan de Silva, spoke to the Sunday Observer on the most dominant
strains in the dengue epidemic in Sri Lanka, and how the virus was
isolated for the first time.
Q. Despite a slight decline in the number of dengue cases in
Sri Lanka, it is evident we are still experiencing near-epidemic
proportions. Have any new strains in the virus caused this recent surge?
A. No. We're still experiencing the same dominant dengue 1
sero type strain which started the epidemic in 2009.
However there is a very small amount of a new dengue strain - Dengue
4 sero type.
There are four main dengue sero types.
The dominant type that we now see in our research with the Health
Ministry's Dengue surveillance unit, is Dengue sero type 1. We were
doing a cohort study with the Epidemiology Unit in 2007 and 2008 where
we saw all four strains and then a sudden shift to dengue sero type 1.
Q. Where do these dengue strains come from?
A. That was a big question for us scientists at Genetech
Research Institute(GRI) as well We decided to investigate further and
locate the source from where these dengue strains that were causing so
many health problems in our country, were coming. Was it from our own
country, or did it arrive from a foreign country, wec wondered.
Q. What did you find?
A. We began a two year long project that culminated in a
publication in the American Journal of Tropical Medicine and Hygiene
(impact factor 2.53). An e print version was published on May 5, 2014
with the formal publication pending on availability of journal space.
The result was somewhat surprising to the scientists themselves.
We found that the dominant Dengue 1 serotype strain that has caused
many deaths and multiple problems in Sri Lanka most probably arrived
from China in 2007.
It had travelled from Thailand to China, then to Sri Lanka and
further gone on to Singapore and Pakistan to create more epidemics in
those countries.
Q. Could you give us a summary or abstract of that
publication?
A. It reads as follows: "A team led by Dr Dharshan de Silva
collaborated with scientists at University of Pennsylvania (UPenn),
Philadelphia, USA, University of Colombo and physicians in the Ministry
of Health to answer this question. Dr Karen Ocwieja an MD/PhD candidate
at that time (she completed her degrees since then) arrived in Sri Lanka
(GRI) in early 2012 for some research work.
While GRI scientists in collaboration with the Epidemiology Unit,
Ministry of Health and others had already identified the dominant Dengue
1 serotype (EID publication reference), they lacked the know how to do
the sophisticated mathematical analysis to trace the phylogeography (to
understand where it came from) of the strain. Dr Ocwieja had this
expertise.
 During her time in Sri Lanka she worked very closely with the other
scientists at Genetech to sequence the full length of the dengue
strains, which had been isolated in Sri Lanka. During her time in Sri Lanka she worked very closely with the other
scientists at Genetech to sequence the full length of the dengue
strains, which had been isolated in Sri Lanka.
In other words the genome of the dengue virus was fully deciphered.
This allowed us to compare our DEN1 genome with others found across the
rest of the world.
A few other scientists at UPenn gave their expertise in analysis of
this data. Furthermore, this coincides with the arrival of several
hundred Chinese workers for infrastructure projects in Sri Lanka during
2007.
This work then underwent rigorous review at the AJTMH journal and was
finally accepted for publication in May 2014.
Q. You say that this DENI strain is still the dominant one
circulating in Colombo.
A. Yes further investigation by GRI scientists strongly
suggests that this DEN1 strain is still the dominant one circulating in
Colombo, Sri Lanka up to date.
Q. What is so special about this virus?
A. What is so special about this virus is that it is so
infectious that it creates epidemics wherever it lands.
Q. Do you know why?
A. No. We need to research further to understand why this is
so.
Q. Tell us how you this research was done.
A. As I mentioned, in early 2012 we had a scientist from the
University of Pennsylvania, US, Dr Ocweija who helped us.
What we did was to first isolate the virus and sequence the RNA (
Ribonuclaic Acid) and analyse it using sophisticated mathematical
analysis to trace the biology of it and see where it came from.
Then we ran it on the BEAST soft ware and came up with the results
which we published.
Q. How is the virus isolated
A. We take samples of dengue patients blood and add them to
mosquito cells. The virus then grows in the cells.
Then we take it and do the RNA followed by sequencing and analysing
with sophisticated lab technology tools.
Q. What did the RNA sequence reveal?
A. We were able to say which country the virus originated from. All
viruses travel around the world and we were able to trace the route of
the dengue virus before its arrival to Sri Lanka. We found that it was
the same dengue virus that had caused epidemics in China and Thailand.
Then we did a further analysis to verify from which of these two
countries it had spread to Sri Lanka.
Q. So which was it? China? Or Thailand?
A. Using the BEAST software, we found it first came to Sri
Lanka in approximately 2007.
Around that time we had several Chinese workers in Sri Lanka working
on the Hambantota project and the cola plant at Norocholi. Further
investigations proved another eye opener for us. Probing further, we
found that it actually started in Cambodia in Vietnam, then came to
Thailand, then to China before coming to Sri Lanka.
Q. Did it go to any other countries from here?
A. To Pakistan and Singapore. There may have been others as
well. But only the countries mentioned had similar labs to do the
analysis.
Q. Why is this strain still dominant in Sri Lanka after nearly
five years?
A. We don't know. We are still investigating.
Q. Does this new breakthrough in knowledge offer new hope for
dengue patients?
A. At present there is still no vaccine for dengue patients.
But it will definitely enhance surveillance of the disease and help us
to prepare ourselves for another outbreak or epidemic. If we had known
that this virulent virus had come to out country in 2007, we may have
been better prepared to face that challenge. We are also doing
immunological studies to shed more light on the subject.
Q. What about the older strains prior to 2000?
A. We don't have any records unfortuntely. But it is very
important that due to the frequency of the epidemics, we set up a Virus
Repository Bank. We are already talking to the Medical Research
Institute and the government to help us start one.
Q. What will be its function?
A. It will store valuable data for researchers to do proper
and more thorough analysis on dengue in future.
Q. Any other strategies recently adopted for Dengue
Surveillance?
A. Right now our surveillance is mostly confined to Colombo.
We need to monitor the spread of the virus island-wide. The Health
Ministry is currently trying to isolate high risk areas and carry out
surveillance. We are ready to help.
Q. Can stem cell therapy or gene therapy help to cure dengue
eventually?
A. Not at present. Proper fluid management under well trained
doctors is our best and only option for serious cases like Dengue
Haemorrhagic Fever. But in the large majority of cases, most patients
don't have any complications, and don't need hospitalisation.
Breakthroughs in ovarian cancer research
Scientists have found new clues to early detection and personalised
treatment of ovarian cancer, currently one of the most difficult cancers
to diagnose early due to the lack of symptoms that are unique to the
illness.
There are three predominant cancers that affect women - breast,
ovarian and womb cancer. Of the three, ovarian cancer is of the greatest
concern as it is usually diagnosed only at an advanced stage due to the
absence of clear early warning symptoms. Successful treatment is
difficult at this late stage, resulting in high mortality rates. Ovarian
cancer has increased in prevalence in Singapore as well as other
developed countries recently. It is now the fifth most common cancer in
Singapore amongst women, with about 280 cases diagnosed annually and 90
deaths per year1.
IMB scientists have successfully identified a biomarker of ovarian
stem cells, which may allow for earlier detection of ovarian cancer and
thus allow treatment at an early stage of the illness.
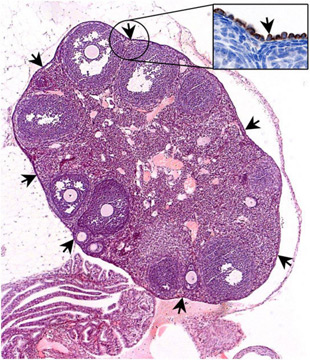 The team has identified a molecule, known as Lgr5, on a subset of
cells in the ovarian surface epithelium2 . Lgr5 has been previously used
to identify stem cells in other tissues including the intestine and
stomach, but this is the first time that scientists have successfully
located this important biomarker in the ovary. In doing so, they have
unearthed a new population of epithelial stem cells in the ovary which
produce Lgr5 and control the development of the ovary. Using Lgr5 as a
biomarker of ovarian stem cells, ovarian cancer can potentially be
detected earlier, allowing for more effective treatment at an early
stage of the illness. The team has identified a molecule, known as Lgr5, on a subset of
cells in the ovarian surface epithelium2 . Lgr5 has been previously used
to identify stem cells in other tissues including the intestine and
stomach, but this is the first time that scientists have successfully
located this important biomarker in the ovary. In doing so, they have
unearthed a new population of epithelial stem cells in the ovary which
produce Lgr5 and control the development of the ovary. Using Lgr5 as a
biomarker of ovarian stem cells, ovarian cancer can potentially be
detected earlier, allowing for more effective treatment at an early
stage of the illness.
Of the different types of ovarian cancers detected, high-grade serous
ovarian carcinoma (HG-SOC) is the most prevalent of epithelial ovarian
cancers3.
It has also proven to be one of the most lethal ovarian cancers, with
only 30 percent of such patients surviving more than five years after
diagnosis4 . HG-SOC remains poorly understood, with a lack of biomarkers
identified for clinical use, from diagnosis to prognosis of patient
survival rates.
By applying bioinformatics analysis on big cancer genomics data5 ,
BII scientists were able to identify genes whose mutation status could
be used for prognosis and development of personalised treatment for
HG-SOC.
The gene, Checkpoint inase 2 (CHEK2), has been identified as an
effective prognostic marker of patient survival. HG-SOC patients with
mutations in this gene succumbed to the disease within five years of
diagnosis, possibly because CHEK2 mutations were associated with poor
response to existing cancer therapies.
Mortality after diagnosis currently remains high, as patients receive
similar treatment options of chemotherapy and radiotherapy
despite the diverse nature of tumour cells within tumours and across
different tumour samples. With these findings, personalised medicine for
ovarian cancer could be developed, with targeted treatment that would be
optimised for subgroups of patients.
Prof Sir David Lane, said, "These findings show how the various
research institutes offer their expertise in developing new approaches
to examine different aspects of the same disease that have not been
successfully studied before, such as ovarian cancer.
The diverse capabilities and knowledge of our scientists allows us to
investigate diseases holistically, from diagnosis to treatment."
- medicalxpress
Link possible between stroke and neck manipulation therapy
The American Heart Association (AHA) has published a statement in
which they say there may be an association between stroke and therapy
involving neck manipulation, although they are unable to confirm whether
neck manipulation causes stroke or not.
This continues a debate that has been ongoing in recent years, in
which various experts have argued over the merits and shortcomings of
neck manipulation within therapy.
 Ischemic strokes are the most common form of stroke, occurring when
arteries connected to the brain become narrowed or blocked. Ischemic strokes are the most common form of stroke, occurring when
arteries connected to the brain become narrowed or blocked.
Neck manipulation has been associated with a risk of cervical artery
dissection, a form of arterial tear that is believed to be an important
cause of stroke in young and middle-aged adults.
Cervical artery dissection
A cervical artery dissection (CD) is a small tear in the layers of
walls in the arteries in the neck.
If the tear becomes dislodged into the bloodstream, it can form a
clot and cause an ischemic stroke by blocking one of the blood vessels
in the brain.
Dr. José Biller, lead author of the statement, explains how these
dissections can occur:
"Most dissections involve some trauma, stretch or mechanical stress.
Sudden movements that can hyperextend or rotate the neck - such as
whiplash, certain sports movements, or even violent coughing or vomiting
- can result in CD, even if they are deemed inconsequential by the
patient."
Some of the techniques used within neck manipulation therapy enact
these sudden movements, by extending and rotating the neck and at times
involving forceful thrusting.
The relationship between CD and neck manipulation therapies came to
light after case control studies were carried out. However, these
investigations are not designed to prove any cause and effect. As a
result, it is unclear whether there are other factors involved that
could explain the link.
"Although a cause-and-effect relationship between these therapies and
CD has not been established and the risk is probably low, CD can result
in serious neurological injury," said Dr. Biller. "Patients should be
informed of this association before undergoing neck manipulation.
Uncertainty remains
One reason the relationship between CD and neck manipulation is
tricky to evaluate is that one of the symptoms of CD is neck pain, which
can precede a stroke by several days. This neck pain may lead people to
seek treatment such as neck manipulation in order to relieve their
symptoms.
- MNT
Ways to find your happy place when stressed
There's sad news in the study of happiness.
Rest assured, there is a happy ending, though. University of
Cincinnati research on perceived happiness shows that many college
students are stressed out and aren't coping.
This is despite the fact that there are simple ways for students to
relieve stress and feel happier, says Keith King, professor and
coordinator of UC's Health Promotion and Education Program. The trouble
is, they don't use them enough.
 "We have a whole array of different stress-management techniques
college students can use and that we teach, but they're not using them. "We have a whole array of different stress-management techniques
college students can use and that we teach, but they're not using them.
That contributes to their stress levels, which contributes to their
unhappiness," King says. King says many simple and effective techniques
exist for managing stress.
He suggests a few immediate and long-term methods for soothing frayed
nerves.
Immediate actions
Stop, pause and breathe: "In the moment when you're stressed, you
need to slow down, you pause, you take some deep breaths. Maybe you
count backwards from 10. Those types of things calm everything down and
slow it down."
See the bigger picture: "Try to see the bigger picture. Is what
you're experiencing really that big of a deal or not?" Contact a friend:
"Everyone has phones on them. Call your buddy and let him know what's
going on so you can express those feelings and get them off you as
quickly as possible."
Long-term actions
Diet and exercise: "People who eat healthy and exercise tend to have
lower stress levels. Exercise allows for some of that negative energy to
get burned off. Eating healthy helps individuals avoid feeling weighted
down."
Daily "me time": "Take time out of the day that's your time. It could
be just 10 minutes. Go outside and walk, just enjoy something for you.
If you hate exercising, then do something you enjoy. That's
paramount."
Remember to H.A.L.T.: "Make sure you're not Hungry, you're not Angry,
you're not Lonely and you're not Tired.
If you can take care of those four things, you're significantly more
likely to be unstressed." King and fellow UC researchers Ashley Merianos,
Rebecca Vidourek and Meha Singh based their study on an anonymous,
voluntary survey taken by 498 students assessing their overall happiness
and stress level.
Results showed that students who reported low perceived happiness
felt higher stress levels and lower emotional closeness to others.
- MNT |







")






