|

Fight dengue with a clean environment
By Carol Aloysius
A relentless surge in the number of dengue cases underscores the
dengue menace is still very real and in fact escalating by the day. This
year alone over 285 suspected cases have been reported countrywide -
over 80 percent positive. Last Saturday, two more persons died from
dengue in Katthankudi bringing the total to nearly 15 since January, the
victims being mostly children.
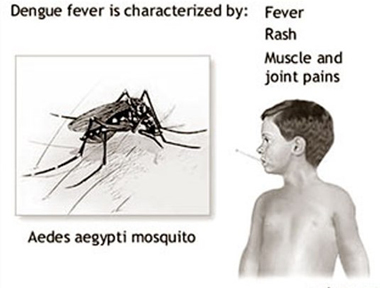
The dengue mosquito (Aedes egypti) survives by feeding on the blood
of several humans. This very active small black mosquito which bites
mainly in the mornings and evenings, lays between 100-200 eggs at a
time, in its short life span.
 With the Health Ministry continuing to battle against the rising toll
of lives, and the grave complications that dengue can bring with it,
their call for clean environments free of dengue breeding grounds is now
loud and clear. The Health of the Epidemiology Unit, Dr Paba
Palihawadana, MOH’s and Public Health Inspectors doing house to house
inspections while continuing their on going anti dengue activities, have
reiterated their frequent appeals to the public: “For God’s sake, keep
your environments clean. Don’t litter your gardens with discarded
plastic containers and lunch sheets. Don’t throw your coconut shells
where even the tiniest collection of rainwater can cause the larvae of
the mosquito to hatch. Clean your gutters. If you can’t do this at least
every week, get rid of them. Mend your broken drains. And make sure that
not just your premises, but those of your immediate neighbours are clean
since the dengue mosquito is basically a neighbourhood creature which
can fly about 150 metres.” With the Health Ministry continuing to battle against the rising toll
of lives, and the grave complications that dengue can bring with it,
their call for clean environments free of dengue breeding grounds is now
loud and clear. The Health of the Epidemiology Unit, Dr Paba
Palihawadana, MOH’s and Public Health Inspectors doing house to house
inspections while continuing their on going anti dengue activities, have
reiterated their frequent appeals to the public: “For God’s sake, keep
your environments clean. Don’t litter your gardens with discarded
plastic containers and lunch sheets. Don’t throw your coconut shells
where even the tiniest collection of rainwater can cause the larvae of
the mosquito to hatch. Clean your gutters. If you can’t do this at least
every week, get rid of them. Mend your broken drains. And make sure that
not just your premises, but those of your immediate neighbours are clean
since the dengue mosquito is basically a neighbourhood creature which
can fly about 150 metres.”
Since the Western Province has the highest incidence of Dengue the
Sunday Observer spoke to the Chief Medical Officer in charge of three
municipal areas - Dehiwela, Mt Lavinia and Ratmalana, to tell us more
about the disease, how to detect it, treat it and most importantly
prevent it.
Following are excerpts of the interview with Dr INDIKA ELLAWELA.
Q. What is dengue?
A. It is an infection caused a virus. The virus is transmitted
by Aedes aegypti and Aedes albopictus.
Q. When a patient gets an attack of dengue is he resistant to
the disease thereafter?
A. There are four subtypes of the virus: DEN 1, DEN 2, DEN 3,
DEN4. Therefore a human can contract dengue fever four times during the
life time.
Q. What do you know about Dengue Mosquito?
A. It’s a very active small black mosquito. Female Aedes
mosquito is the vector of dengue. It bites several people to get one
blood meal. It bites mainly the mornings and evenings. The life span of
an adult Aedes mosquito is around 2-4 weeks. It lays eggs around four
times during the life span. It lays around 100 - 200 eggs at a time, The
eggs are sticky, therefore difficult to remove. It takes 7-11 days to
emerge an adult mosquito from the egg. The eggs can remain live up to 1
year in dry conditions and hatch on contact with water.
Q. Who are those most at risk?
A. The risk groups are:
??Children - As the Aedes mosquitoes are day bitters, school going
children are more vulnerable to get infected with dengue virus
*Elders
*Obese people
*Persons with chronic diseases (eg: Bronchial asthma, diabetes)
*Persons with immunodeficiency.
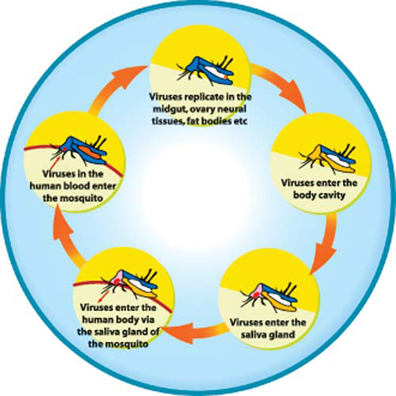
Q. What happens when someone is infected with Dengue virus?
A. Around 90 percent of people infected with dengue virus for
the first time do not show symptoms and signs. But they too have Dengue
virus in their blood for 5-7 days. During this period if they are bitten
by mosquitoes, the virus can enter into these mosquitoes with the blood
meal and multiply within the mosquitoes. These infected mosquitoes can
transmit virus to healthy people. Accordingly you may have already
contracted Dengue fever for the first time with or without your
knowledge. Once the virus enters your body it will take about 7-10 days
to develop symptoms and signs.
If a person infected with one subtype of Dengue virus, antibodies are
formed against that subtype and he/she will be protected for that
particular virus subtype in the future, but not protected for remaining
three subtypes. Therefore they can contract Dengue fever again by any of
other three subtypes of virus.
When a person contracted Dengue fever for the 2nd, 3rd, or 4th time
disease is more severe than first episode and possibility of developing
Dengue Haemorrhagic fever is high.
Q. What are the different types of dengue commonly found in
Sri Lanka?
A. Many patients infected with dengue virus remain
asymptomatic. Others can develop a febrile illness one of the following
types:
Undifferentiated fever
 Dengue Fever (DF) Dengue Fever (DF)
Dengue Haemorragic Fever (DHF) - most serious.
In Dengue Haemorrhagic Fever, the patient goes through different
phases.
1. Fever phase
2. Critical (Leakage) phase
3. Convalescent (Recovery) phase
Q. How long does the fever phase last?
A. The fever phase usually lasts for 2-7 days’ during which
patient can have body aches and pain, muscle pain, severe headache, pain
behind the eyes, vomiting and rash (Red colour).
Sometimes there can be sore throat and congestion of eyes (red eyes).
These symptoms are similar in both dengue fever and dengue haemorrhagic
fever.
Sometimes the fever can be subside abruptly, but the patient’s
condition deteriorates and develops into complications of dengue fever.
Therefore, monitoring of patient’s general condition, adequate rest
and fluid intake is essential to prevent complications.
Critical phase
The critical phase is usually evident after the third day of fever
and the symptoms and signs are due to plasma (liquid part of the blood)
leakage through blood vessels due to the adverse effects of the virus on
walls of blood vessels.
This will cause thickening of blood and circulatory failure leading
to shock.
Due to the same reason, there is reduction of blood supply to
essential organs in the body causing failure of vital organs.
The patient can die of either of these complications or by both.
Early detection and prompt treatments can prevent death’. Reduction of
platelets however is usually not a reason for death in dengue patients.
Convalescent (Recovery) phase
During the recovery phase, plasma which leaked out of the blood
vessels will re-enter to the blood stream and patient’s condition
improves gradually. Regaining appetite and improvement of urine output
are some indicators of recovery. During this phase too it is necessary
to take adequate rest and food.
Q. When or how does one suspect dengue illness?
A. Presence of the following clinical features with acute
onset of fever.
Headache and retro-orbital pain
Nausea and vomiting
Joint pain (Arthralgia) and muscle pain (myalgia)
Rash
Laboratory findings
Low white cell counts (Leucopenia - WBC <5000/mm3)
Low platelet count (?150,000/ mm3)
Rising Haematocrit (HCT- 5-10%)
Q. How is the fever managed? Can it be managed at home?
A. If the patient is treated at home, make sure he/she is
given adequate oral fluid intake (oral rehydration fluid, king coconut
water, other fruit juices, kanji, soup) - Avoid giving red and brown
drinks. Make sure he gets adequate physical rest
* Sponge him with tepid water to bring down the fever.
* If drugs are to be taken, take only paracetamol (10-15mg/kg/dose-
Do not exceed 60mg/kg/24 hours)
* Anti-emetics if necessary
*Avoid other analgesics in any form and steroids
* Review daily with Full Blood Count (FBC)
First FBC should be done on the third day of fever and daily
thereafter if the platelet count is >150,000/mm3; twice daily if
<150,000/mm3)
However, a FBC is recommended on the first day of fever during
infancy and in patients with major medical problems
Q. What are the warning signs of the onset of DHF?
A. Inability to tolerate oral fluids
*Refuse to eat or drink
*Feeling extremely thirsty
*Severe abdominal pain/ vomiting
*Cold and clammy extremities
*Bleeding manifestations
*Not passing urine for more than six hours
*Behavioural changes eg: Confusion, restlessness, lethargy,
irritability
Q. When should a patient be taken to hospital?
A. All patients with a platelet count of ?100,000/ mm3
*?All patients with above mentioned warning signs
*?Infants, obese patients, patients with major medical problems,
patients with adverse social circumstances (living alone, living far
from health care facility without reliable transport, unreliable
patients also should be admitted.
Q. Treatment given at the hospital?
A. Mortality from dengue can be reduced by timely management.
Appropriate clinical management, which involves early clinical and
laboratory diagnosis, intravenous rehydration and staff training.
Q. How can dengue be prevented?
A. A vaccine against dengue fever is in the process of being
developed.
Chemical control is also effective in controlling mosquito
population. Insecticides can be used to kill mosquito larvae or adult
mosquitoes. The use of insecticides is recommended in emergency
situations during dengue epidemics. However, on a regular basis use of
chemical methods can make mosquitoes to develop resistance to
insecticides. In addition, insecticides are expensive and harmful to
human when using high doses.
Mosquito repellants which contain DEET, Picaridin or oil of
lemon/eucalyptus
Precautions to avoid being bitten by mosquitoes
-Keep unscreened windows closed
One practical and recommended environmental management strategy
Is to eliminate unnecessary breeding habitats that collect water
(plastic jars, bottles, cans, tires) in which Aedes aegypti mosquito can
lay the eggs. This strategy is called ‘source reduction’.
Q. Your message to the public?
A. Community based approaches must go hand in hand with
educational initiatives that teach people about mosquito vectors and the
risk of having mosquito breeding habitats near their houses. Educational
initiatives can encourage people to take an active role in participating
in source reduction. Communities must understand that behavioural
changes are the most effective way to control dengue.
As all of us at risk to dengue virus infection, pay attention to roof
gutters because 20 percent of breeding places are found in those sites.
If you have fever…
* Suspect it as dengue fever
*Take adequate rest
*Avoid sending children to schools, adults should not to go work
*Exempt from strenuous exercise/work
*Take only Paracetamol in recommended doses for fever
* Avoid other fever reducing drugs in any form (tablets, syrups,
suppositories etc) such as Diclofenac Sodium, Mefenemic Acid, Aspirin
and Ibuprofen
*If fever continues for more than two days, consult a qualified
doctor.
*?Drink adequate amount of liquids (oral rehydration fluid-Jeewani,
king coconut water, other fruit juices, kanji, soup)
*Avoid taking red/brown colour foods or drinks which can change the
colour of stools/urine.
Q. Any other comments?
A. We have noticed that more than 75 percent Dengue cases, the
source of infection is inside their premises and people still believe
that this source reduction exercise has to be carried out by health
officials. People have to realise that regular cleaning of their
premises both inside and outside is their own responsibility.
Researchers determine how the brain controls robotic grasping tools
Findings could lead to assistive technologies benefitting the
disabled
Grasping an object involves a complex network of brain functions.
First, visual cues are processed in specialized areas of the brain.
Then, other areas of the brain use these signals to control the hands to
reach for and manipulate the desired object.
 New findings from researchers at the University of Missouri suggest
that the cerebellum, a region of the brain that has changed very little
over time, may play a critical role. Findings could lead to advancements
in assistive technologies benefiting the disabled. New findings from researchers at the University of Missouri suggest
that the cerebellum, a region of the brain that has changed very little
over time, may play a critical role. Findings could lead to advancements
in assistive technologies benefiting the disabled.
“We live in a world of advanced technology in which a button can move
a crane or open a door,” said Scott Frey, professor of psychological
sciences in the College of Arts and Science and director of the Brain
Imaging Center at MU.
“For those with disabilities, assistive technologies, such as robotic
arms or sensors inserted in the brain, make it possible to accomplish
actions like grasping with the press of a button or directly through
brain activity; however, little is known about how the human brain
adapts to these technologies.
We found that the brain didn't necessarily evolve to control modern
robotic arms, but rather the cerebellum, an ancient portion of our brain
that has remained relatively unchanged, plays a vital role in helping us
reach and grasp with these tools - often with only minimal training.”
Tasks
In the study, participants completed a series of ordinary reaching
and grasping tasks involving colored wooden blocks. Regions of the brain
were monitored by functional magnetic resonance imaging (fMRI). Then, in
a training session, participants were introduced to a robotic arm that
performed the same reaching and grasping tasks when they pressed
specific buttons. Participants were told that the next day's tasks would
involve their controlling the robot remotely by video feed from within
an MRI scanner.
“We found evidence that the brain is very flexible and can be rapidly
conditioned to associate new consequences with a variety of movements,”
Frey said. “Pressing a button is a very simple act that does not
naturally result in grasping.
Nevertheless, after subjects learned that pressing one button would
result in grasping objects with a robotic arm, this same movement
resulted in a dramatically different pattern of brain activity than
pressing an identical button known by them to have no effect on the
robot's behavior. Localized activity within the cauliflower-shaped
cerebellum, or ‘small brain’ sitting toward the back of the head,
increased dramatically.
These findings suggests that we might look to the cerebellum when
seeking potential targets for brain-controlled interfaces.”
MNT
One in two people ‘will be diagnosed with cancer’ at some point in
their lives
One in two people will develop a cancer at some point in their lives,
experts now estimate.
Previous calculations that indicated cancer will affect just over one
in three people were underestimating the scale of the disease, according
to a new analysis by Cancer Research UK.
 However, because of advances in treatment and early detection, more
people are now surviving cancer. However, because of advances in treatment and early detection, more
people are now surviving cancer.
Two-thirds of the increase in risk can be attributed to the fact we
are now living longer, and cancer is a disease that becomes more likely
the older we get. The additional third is down to changes in lifestyle,
CRUK said.
The study calculates the lifetime risk of cancer for men born in the
UK in 1960 is 53.5 per cent and for women 47.55 per cent, averaging at
50.5 per cent. The risk is likely to increase for people born after
1960, and CRUK said it was confident in predicting that this meant at
least half the population can now expect to get cancer.
“Cancer is primarily a disease of old age, with more than 60 per cent
of all cases diagnosed in people aged over 65,” said cancer specialist
Prof Peter Sasieni, who led the new study. “If people live long enough
then most will get cancer at some point.
“But there’s a lot we can do to make it less likely – like giving up
smoking, being more active, drinking less alcohol and maintaining a
healthy weight.” The new calculation does not mean that each individual
in the UK has 50/50 chance of getting cancer, as risk varies
significantly according to age, weight, diet, as well as a range of
lifestyle, genetic and environmental factors.
Recent estimates suggest that half of people who get cancer now
survive the disease for 10 years or more - so it is projected that
despite more cases, the number of deaths attributable to cancer will
remain stable at around one in four.
Changes in lifestyle that have contributed to the increase in cancer
risk include an increase in obesity, which is linked to a number of
cancers and is projected to continue rising. Higher consumption of red
and processed meats is also linked to a rise in bowel cancer. Other
factors include an increase in the culture of using sunbeds and
sunbathing, which has increased incidence of skin cancer, while women
having babies later and breastfeeding less is also raising their chance
of developing breast cancer. As well as this, more cancers are being
detected by screening programs.
CRUK’s chief executive Harpal Kumar, said that the NHS faced a
challenge to ensure it was “fit to cope” with the increase in cases. “If
the NHS doesn’t act and invest now, we will face a crisis in the future
- with outcomes from cancer going backwards,” he said. Cancer services
are already coming under increased strain, with the NHS in England
having missed key waiting time targets for cancer patients for the first
time last year.
- The Independent
|









")




