 |
 |
| |||
|
|
|||||||||||||||||||
|
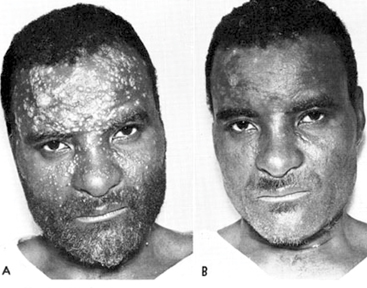
Q. Leprosy was a disease that killed thousands of persons in Sri Lanka in the 1930s. Your comments? A. Leprosy was never a lethal disease that killed thousands during any era. It probably affected few thousands every year, eventually leading to proportionately more people disabled, compared to now. Q. Is the picture as grim in Sri Lanka today? A. Leprosy remains a problem even today with around 2,000 new leprosy patients diagnosed per year for the past 15 years. Q. Do you consider this a disease of the past now? A. No. It is still remains very much a disease of the present mainly due to the fact that there 2,000 new leprosy cases reported every year and there nearly 180 new patients with grade 2 disability reported every year. Q. If so, why is it that new cases are emerging even now? A. There have always been more than 1,500 cases reported in Sri Lanka over the past. For the past 15 years there have been 2,000 new leprosy cases reported every year and there are nearly 180 new patients with grade 2 disability reported every year and nearly 180 new child cases reported each year. Q. Many still don't know much about this disease since the number of cases has dropped significantly. So tell us, what is leprosy in medical terms? A. Leprosy is a chronic infectious disease caused by the bacteria which affects the skin and the nerves. Transmission of leprosy is by droplet infection. Disease is transmitted from human to human and there is no reservoir or a vector. The disease is not spread by a person who has taken treatment. Leprosy disease is easily diagnosable - treatable and curable. Diagnosis is mainly a clinical one. Major issue associated with leprosy is development of disabilities leading to loss of productivity and social stigma. These disabilities result from reactions occurring at any stage of the disease even after completion of treatment and could be prevented by early detection and treatment. Q. What causes it? A bacteria? Virus? Insects? Is it genetic related or due to lifestyle changes or poor nutrition, poor personal hygiene? A. It’s a bacteria namely mycobacterium leprae. Some of the identified risk factors include overcrowding, poor nutrition. Q. Are there different types of leprosy? If so, what are they? A. There are basically two different types of leprosy. Multibacillary (or infectious) type and Paucybacillary (or non infectious) type depending on the clinical features. Q. Is the severity of the disease the same in all these types? A. No. Multibacillary patients are more severely affected due to poor immunological reaction from the body. They are also at more risk of developing complications and disability. Q. What is the most severe type? What are the symptoms of this type? A. Most severe form is called lepromatous leprosy where features include leonine facis, numbness of hands and feet and nasal stuffiness. Q. What is the mildest? What are the symptoms? A. Its called Indeterminate type of leprosy where there is only a hypo-pigmented patches sometime even without anaesthesia. Q. Can Leprosy be mistaken for some other skin ailment e.g. ‘aluhan’ (pitysiriasis)? A. Yes, some conditions such as pityriasis rosea, post inflammatory hypopigmentation and photodermetitis mimic pucibacillary leprosy hypo pigmented patch. However, most of the skin lesions you see in many other skin conditions such as psoriasis etc can be similar to leprosy lesions. Q. What organs are most affected by the disease? Which sites are vulnerable when such organs are affected? Neck? Hands? Elbows? Legs? A. Mainly skin and peripheral nerves. Q. Is leprosy infectious? Can it be transmitted to another person? If so how? Sputum? Close contact? A. It is spread through droplets from infected individuals with Multibacillary (or infectious) type who are not taking treatment to healthy individuals through the respiratory tract. However it is not highly infectious. It takes prolonged exposure for a long time for a healthy individual to get infected. Q. How is leprosy detected? In the tissues? A. Its mainly a clinical diagnosis depending on skin lesions. Sometimes skin smear and biopsies are taken in doubtful cases and for follow-up purposes. Q. What are the complications of the disease? Loss of sensation? Deformities? What happens when you lose sensation or feeling of pain? A. Main complications are due to reaction leading to nerve damage causing loss of sensations and muscle weakness which manifest as deformities and sometimes pressure ulcers due to anaesthesia Q. What kind of deformities can occur? A. Clawing of the hand, foot drop and neuropathic ulcers are the commonest. Q. Is there hope to patients compared to the past? A. Yes, compared to an era without antibiotics there are effective drugs which can completely cure leprosy when taken properly after early diagnosis. Q. What is Multiple Drug Therapy (MDT)? A. It is a combination of more than one antibiotics. For Paucybacillary (or non infectious) patients it is dapsone and rifampicin for Multibacillary (or infectious) type patients it is dapsone, rifampicin and clofazamine Q. If treated early can it stop the disease from progressing? A. Yes. Complete cure can be achieved. Q. Can it rectify deformities already caused? A. Yes, if they present within a short time within onset (six months) it can be 100 percent reversed with treatment and rehabilitation. Even those who present later can receive some sort of recovery after rehabilitation and reconstructive surgery. Q. For how long should one take treatment? Does the duration depend on the type of leprosy? A. Six months for and Paucybacillary (or non infectious) And 12 months for Multibacillary (or infectious) type. Q. Can treatment be done at home? A. Yes. It is usually taken at home. Once in a month they have to go to the clinic to get the card and observed treatment. Q. Where can patients get treatment? Do all hospitals have leprosy units? Or only a few? A. Treatment is given free of charge from government hospitals where a dermatology clinic is functioning. Q. What are the main obstacles to leprosy prevention? A. Main obstacles include late detection patients and patients not coming forward for treatment due to stigma and lack of public awareness that leprosy is still prevalent. Q. What role does 1) lack of information 2) myths about leprosy play in preventing it? A. 1) If you don’t know that you have leprosy, and you don’t know that you have the signs and symptoms, you will not go for treatment. 2) Myths about leprosy play leads to patients hiding away thinking that leprosy is a dangerous disease which should be hidden from everybody without coming for treatment. Q. Apart from medical personnel, can people working at grassroots level such as midwives, PHIs, family health workers help in detection? If so, does the Health Ministry have a training program for them? A. Yes. Already they are given training at district level for diagnosis of leprosy to detect cases in the periphery and send for treatment. Q. What is the vision of the Elimination of Leprosy program initiated by the Global Alliance on Leprosy? A. The vision in the Global leprosy program now is a leprosy free world. The aim is to reduce the burden of leprosy and ultimately move towards a leprosy-free world. Q. When does the Health Ministry hope to eliminate leprosy 100 percent from Sri Lanka? A. The main aim is to work towards further reducing leprosy burden in the country, eventually leading to a leprosy-free Sri Lanka. This will take some time due to the chronic nature of illness and because incubation period can be as long as 20 - 30 years. Q. Your message to the public? A. Leprosy is curable. It’s not a disease to be feared. When diagnosed early and treatment is taken, it is completely curable. Treatment is available free at government hospitals. Your privacy online: Health information at serious risk of abuseThere is a significant risk to your privacy whenever you visit a health-related web page. An analysis of over 80,000 such web pages shows that nine out of 10 visits result in personal health information being leaked to third parties, including online advertisers and data brokers. This puts users are risk for two significant reasons: first, people's health interests may be publicly identified along with their names. This could happen because criminals get ahold of the information, it is accidentally leaked, or data brokers collect and sell the information.
Predictably, those in the “target” category are extended favourable discounts at retailers and advance notice of sales. Given that 62 percent of bankruptcies are the result of medical expenses, it is possible anyone visiting medical websites may be grouped into the “waste” category and denied favourable offers. For individuals, this means profiles are built based on web page visits, potentially resulting in someone being labeled a commercial risk due to the fact that they have used a site like WebMD.com or CDC.gov to look up health information for themselves, a family member, or a friend. Given that data brokers are free to sell any information they collect regarding visits to health websites, those visiting such sites are potentially at risk of being discriminated against by potential employers, retailers, or anybody else with the money to buy the data. These findings are reported in the article “Privacy Implications of Health Information Seeking on the Web,” appearing in the March 2015 issue of Communication of the ACM. Timothy Libert, a doctoral student at the University of Pennsylvania's Annenberg School for Communication wrote the article. He authored a software tool that investigates Hypertext Transfer Protocol (HTTP) requests initiated to third party advertisers and data brokers. He found that 91 percent of health-related web pages initiate HTTP requests to third-parties. Seventy percent of these requests include information about specific symptoms, treatment, or diseases (AIDS and Cancer). The vast majority of these requests go to a handful of online advertisers: Google collects user information from 78 percent of pages, comScore 38 percent, and Facebook 31 percent. Two data brokers, Experian and Acxiom, were also found on thousands of pages. “Google offers a number of services which collect detailed personal information such as a user's personal email (Gmail), work email (Apps for Business), and physical location (Google Maps),” Libert writes. “For those who use Google's social media offering, Google+, a real name is forcefully encouraged. By combining the many types of information held by Google services, it would be fairly trivial for the company to match real identities to “anonymous” web browsing data.” Indeed, in 2014, the The Office of the Privacy Commissioner of Canada found Google to be violating privacy Canadian laws. “Advertisers promise their methods are wholly anonymous and therefore benign,” Libert writes. “Yet identification is now always required for discriminatory behaviour to occur.” He cites a 2013 study where individuals’ names were associated with web searches of a criminal record, simply based on whether someone had a “black name.” “Personal health information - historically protected by the Hippocratic Oath - has suddenly become the property of private corporations who may sell it to the highest bidder or accidentally misuse it to discriminate against the ill,” Libert said. “As health information seeking has moved online, the privacy of a doctor's office has been traded in for the silent intrusion of behavioral tracking.” Online privacy has for some time been a concern. Studies conducted by Annenberg dating back to 1999 indicate wariness among Americans about how their personal information may be used. And slightly more than one in every three Americans even knows that private third-parties can track their visits to health-related websites. Libert points out that the Federal Health Insurance Portability and Accountability Act (HIPPA) is not meant to police business practices by third party commercial entities or data brokers. The field of regulation is widely nonexistent in the U.S., meaning that individuals looking up health information online are left exposed and vulnerable. According to Libert, “Proving privacy harms is always a difficult task. “However, this study demonstrates that data on online health information seeking is being collected by entities not subject to regulation oversight. This information can be inadvertently misused, sold, or even stolen. “Clearly there is a need for discussion with respect to legislation, policies, and oversight to address health privacy in the age of the internet”. MNTStudy shows how the brain can trigger deep sleepScientists have discovered that switching on one area of the brain chemically can trigger a deep sleep. The new study, which explored how sedatives work in the brain's neural pathways, could lead to better remedies for insomnia and more effective anaesthetic drugs.
Following a period of sleep deprivation, the brain triggers a process that leads to a deep recovery sleep. The researchers found that the process that is triggered by the sedatives is very similar. In mice, when the researchers used a chemical to activate only specific neurons in the preoptic hypothalamus, this produced a recovery sleep in the animals. The new research is important because although scientists understand how sedatives bind to certain receptors to cause their desired effects, it had previously been assumed that they had a general effect throughout the brain. The knowledge that one distinct area of the brain triggers this kind of deep sleep paves the way for the development of better targeted sedative drugs and sleeping pills. These new drugs could directly hijack this natural mechanism to work more effectively, with fewer side effects and shorter recovery times. “If you don't sleep for a long period, your body shuts down - almost as if you had taken a drug,” said study co-author Professor Bill Wisden, from the Department of Life Sciences at Imperial College London. “We've shown that sedative drugs trigger the same neurons, making the two types of unconsciousness very similar.” “Although we know that certain sedatives are effective, there are lots of gaps in scientists’ knowledge in terms of precisely what sedatives are doing in the brain. We looked at the class of sedative drugs commonly used for patients undergoing investigative procedures or minor operations, to try and identify the circuitry in the brain that they are affecting,” explained Nick Franks, also from the Department of Life Sciences at Imperial College London. “What we found was really striking. Most people might think that sedative drugs would work by directly shutting down certain neural pathways but actually what happened was that they first switched on one particular area - the preoptic hypothalamus - and this then caused other parts of the brain to shut down.” “Lack of sleep is a really serious problem for many people, such as people suffering from stress or people working irregular shifts, and it affects their physical and mental health” said Prof Wisden. “There are many different sleeping pills available but none of them provide rest that is as restorative as natural sleep. We hope that our new research will ultimately lead to new ways of addressing this problem.” - MNT
|
|




 Second, many online marketers use algorithmic tools which
automatically cluster people into groups with names like “target” and
“waste”.
Second, many online marketers use algorithmic tools which
automatically cluster people into groups with names like “target” and
“waste”.  Scientists found that certain types of sedative drugs work by
‘switching on’ neurons in a particular area of the brain, called the
preoptic hypothalamus. Their work, in mice, showed that it is these
neurons that are responsible for shutting down the areas of the brain
that are inactive during deep sleep.
Scientists found that certain types of sedative drugs work by
‘switching on’ neurons in a particular area of the brain, called the
preoptic hypothalamus. Their work, in mice, showed that it is these
neurons that are responsible for shutting down the areas of the brain
that are inactive during deep sleep. 







")
