World Stroke Day was
on October 29 -:
A stroke in waiting
Urbanization, increase in the ageing population and poor
socio-economic status all mean, more Sri Lankans are at risk of
suffering a brain attack:
by Carol Aloysius
 Stroke is perhaps one of the most debilitating diseases resulting in
long term disability. However, its devastating impacts on the human body
can be minimized if the patient is rushed to the nearest hospital in the
shortest possible time, no sooner he/she gets a stroke (brain attack). Stroke is perhaps one of the most debilitating diseases resulting in
long term disability. However, its devastating impacts on the human body
can be minimized if the patient is rushed to the nearest hospital in the
shortest possible time, no sooner he/she gets a stroke (brain attack).
Here, Consultant Neurologist, Sri Jayewardenepura General Hospital,
Dr Harsha Gunasekara, discusses the risk factors contributing to stroke,
signs to look out for before a stroke and treatment available.
Excerpts…
Q: Stroke is a leading cause of illness and death worldwide and in
Sri Lanka. Has there been a significant increase in the incidence in
recent years? If so why?
A: Stroke is the 3rd leading cause of death and the leading cause of
disability worldwide. In Sri Lanka, Stroke has taken 2nd or 3rd place
for hospital deaths. However, national statistics on Stroke incidence
are not available to date in Sri Lanka. Two community based studies done
in Colombo and Gampaha Districts show that around 1% of the population
develop stroke annually (approximately 200,000 stroke patients per year.
As for why, three major causes in developing countries like ours include
change in lifestyle associated with urbanization, increase in the ageing
population and poor socio-economic status, which hinders successful
strategies for prevention and treatment of stroke.
Q: Are these risk factors similar to those that have caused a surge
in other non-communicable diseases (NCDs) in Sri Lanka?
A: Risk factors for stroke and other NCDs (heart disease, cancer
etc.), are quite similar. The major risk factors for Stroke are smoking,
high blood pressure, diabetes, atrial fibrillation (irregular heart
rhythm which predisposes to stroke) and Carotid artery disease
(narrowing of the major arteries which feed the brain). All these five
major risk factors are modifiable, which means that if you correct them
(for example quitting smoking, treating high blood pressure, diabetes
and irregular heart beat etc.) you can prevent a stroke.
Other modifiable risk factors include obesity, physical inactivity,
high blood cholesterol levels, some heart diseases, use of contraceptive
pill and post-menopausal hormone replacement, diseases which predisposes
to abnormal blood clotting, excessive alcohol consumption, and narcotic
drug use.
 Non-modifiable risk factors include advanced age, male gender, and
family history of stroke, and low birth weight. Non-modifiable risk factors include advanced age, male gender, and
family history of stroke, and low birth weight.
Q: Can Stroke be prevented?
A: Even with most modern treatment facilities, only a third of
patients gain complete recovery from Stroke. Therefore, it’s best to
prevent a Stroke before it develops. This can be done at two levels,
namely ‘primordial prevention’ and ‘primary prevention’. In primordial
prevention, life style modifications are practiced early to prevent
development of Stroke Risk Factors stated above. Primary prevention is
for people with established risk factors, yet not suffered a Stroke
where treatment with medication in addition to life style modifications
is started to prevent a stroke.
The third form of prevention called ‘Secondary Prevention’ is for
patients who have suffered a Stroke or a TIA where anti-platelet
(blood-thinning) treatment is started in addition to the measures used
in primary prevention.
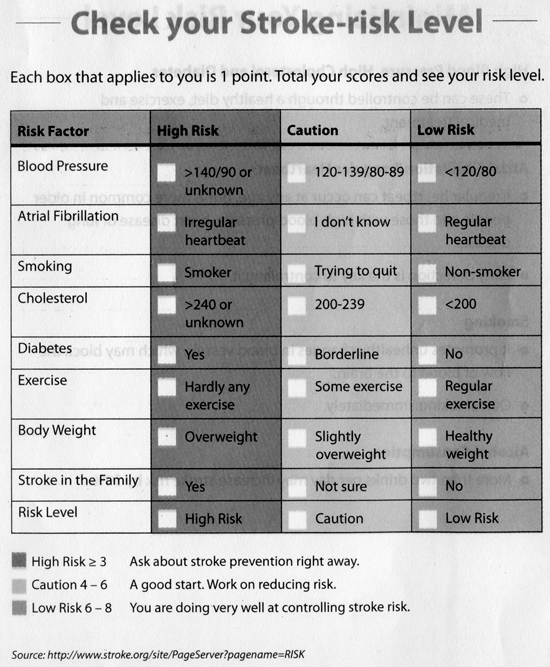
It’s best to adopt the two former methods of prevention and anyone
can assess his or her Stroke risk using a simple scorecard (see the
chart given elsewhere).
Q: How soon should a person be taken to hospital after a stroke?
A: When a person has symptoms of a heart attack, he is taken to the
nearest hospital immediately. The same thing should be done when someone
suffers from stroke. Just as heart attacks occur due to blockage of a
blood vessel feeding the heart muscle, over 85% of Strokes occur due to
blockage of a blood vessel feeding the brain (the rest due to ruptured
blood vessel causing a brain bleed). Stroke is a ‘brain attack’. A
person with symptoms of a suspected Stroke should be taken to the
nearest hospital immediately. There are two main reasons for this.
Firstly, to perform a CT scan to rule out or confirm a brain bleed and
secondly to initiate treatment without delay.
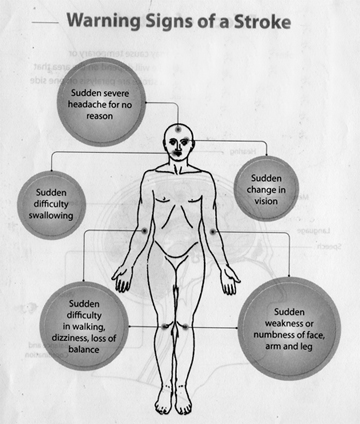
Q: Early symptoms? How do we recognize them?
A: Stroke ‘strikes’ you suddenly, with a wide range of symptoms
depending on the area of the brain affected. The common ones are
numbness or weakness of one side of the body or one limb alone,
disturbance of speech, impaired vision in one eye or double vision,
impaired balance and co-ordination and impaired swallowing and bladder
control. Sometimes headache, vomiting and impaired level of
consciousness can occur especially in the case of a brain bleed.
As remembering all these symptoms is difficult, stroke organizations
have put forward a simple test called FAST – Face, Arm, Speech, Time
which is explained in the diagram.
If any of the 3 checks are positive, the patient should be taken to
the nearest hospital immediately.
 Q: Any other symptoms? Q: Any other symptoms?
A: Around a quarter of patients with Stroke may experience a
Transient Ischemic Attack (TIA or mini Stroke). Here the symptoms of
Stroke last only for a few minutes and then rapidly resolve. This
condition should be given serious consideration and treatment initiated
as it may be the only warning one may get before developing a major
stroke.
Q: What is the first line of treatment?
A: Doctors will first assess the patient to confirm a Stroke and
determine the risk factors, then do investigations including a CT scan.
Initial treatment involves monitoring and controlling the blood pressure
(which should not be too high or too low in the early stages after a
Stroke), blood glucose level, oxygen level, and if needed measures to
reduce brain swelling. Once a brain bleed is ruled out, blood thinning
(anti-platelet) treatment is initiated. Patients will also be given
cholesterol lowering drugs. If the patient is brought to the hospital
and a brain bleed is ruled out within 3 hours, clot buster treatment is
given in a few hospitals where it’s available. In the near this
treatment will be available in most major government hospitals in the
island.
All patients with Stroke should also be assessed and treated for
possible complications such as infections (of the lungs and the urinary
passage), DVT (clots in the leg veins), pressure ulcers and depression.
Stroke patients should be managed with the aim of preventing these
complications which would otherwise adversely affect recovery from
stroke.
Q: What is the next step towards rehabilitating victims?
A: Rehabilitation of a stroke victim requires multidisciplinary
support and is best undertaken in the setting of a Stroke Unit. A Stroke
Unit is a hospital unit (may be separate or part of a ward) that cares
for stroke patients exclusively or almost exclusively, with specially
trained staff and a multidisciplinary approach to treatment and care.
The multidisciplinary team consists of doctors, nurses,
physiotherapists, occupational therapists, speech and language
therapists, psychologists/counsellors and a social worker. It has been
proven that treatment in a Stroke unit improves chances of survival and
reduces both disability and length of hospital stay.
Q: Where are these Units?
A: At the National Hospital Sri Lanka, which was the first of our
Units, in Kurunegala, Kalutara, Ragama Sri Jayewardenepura, Badulla,
Ratnapura, and Anuradhapura hospitals Six more units are being set up
this year.
Q: Any dietary guidelines?
A: The diet should be rich in fruits and vegetables and low-fat dairy
products and reduced saturated and total fat, sugar and salt. Cessation
of smoking and limitation of alcohol intake are essential to prevent
another stroke attack.
Q: Exercise?
A: Guidelines for exercise recommend increased moderate aerobic
physical activity for 150 minutes a week (i.e. 30 minutes a day for 5
days). There is no limitation of the type of aerobic physical activity
as long as the patient can cope with it safely (especially with the aim
of avoiding falls). Supervision and guidance by a physiotherapist or
carer may be needed in the initial period, while close medical
supervision may be required for patients with heart and lung diseases.
Q: How long does it take for a patient to recover?
A: On average after a stroke, one third of patients fully recovers or
will have only minor disability. Another third will be disabled for
life. One third of patients will die, either directly as result of the
stroke or due to one of its complications. Duration of recovery is
variable depending on the severity of stroke, age of the patient,
presence of complications and the setting of post-stroke care.
Majority of patients who do recover usually regain physical functions
and activities of daily living over a period of approximately 2 – 4
weeks. Stroke victims carry a higher risk of developing a second stroke,
irrespective of their level of recovery. Patients should strictly adhere
to advice on lifestyle modifications and take treatment prescribed to
prevent another stroke.
I am a woman; Stroke affects me
Giving their views on the subject at a media discussion at the Health
Education Bureau Friday October 29, two Consultant Neurologists, Dr.
Udaya Ranawaka, President of the National Stroke Association of Sri
Lanka and former President Stroke Association and Consultant
Neurologist, National Hospital Sri Lanka, Dr Padma Gunerathne, said the
theme of this year’s World Stroke Day, was ‘I am a woman; Stroke affects
me, stroke affects everyone’. It had been especially chosen due to
escalation of risk factors, which make women more vulnerable to stroke
than men, they noted, a fact proved statistically. Out of ten stroke
deaths six were likely to be women.
The reasons? Because they live longer than men, and have age related
diseases more frequently than men e.g. hypertension, diabetes, migraines
with visual aura, atrial fibrillation, depression and are more prone to
obesity than men. They also suffer from sex specific risk factors such
as pregnancy, pre-eclampsia, take birth control pills, hormone
replacement therapy, and develop gestational diabetes, cerebral venous
thrombosis.
The doctors also noted that women do not receive the same care that
men with stroke receive, and less rehabilitation than men, although they
responded equally well to the treatment given. The fact that most women
delay going for treatment due to their multiple roles as housewives and
mothers, even after they were alerted to the symptoms, make their
situation worse.
“These gender gaps between men and women with stroke require more
awareness raising and education. There are many gaps which we hope to
fill once our new Centre for stroke activities at the National Stroke
Hospital at Mulleriyawa gets underway soon,” Dr Ranawaka said. |








