Healthy lifestyle cuts Alzheimer's risk
|

Dr. Harsha Gunesekara |
While an aging population puts more Lankans at
risk, pathological changes in the brain probably start 10-20 years
before any visible symptoms of the disease appear. Research has revealed
that lifelong wellness habits and control of other health conditions can
prevent the disease.
by Carol Aloysius
Alzheimer's Disease (AD) has surged in recent years due to several
seemingly divergent factors in today's world where speed is what
matters. Despite on-going research and technical advances on Alzheimers
Disease (AD) globally, these complex factors have collectively combined
to make it one of the least understood diseases in the world.
Memory loss, the most visible symptom is only one aspect of this
debilitating condition. To date, the single cause or causes responsible
for reducing once vibrant, self reliant persons to total dependency,
even to the extent of performing their daily personal chores has yet to
be revealed. Sadly, despite promising results from on-going research,
curing Alzheimer's also continues to remain an elusive dream.
Consultant Neurologist, Sri Jayawardenepura Hospital, Dr. Harsha
Gunesekara shares his views with the Sunday Observer on symptoms to look
for, and treatment options available to Lankan patients
Excerpts...
Q: In your long years of dealing with Alzheimer patients, do
you see a visible increase in the number of cases over the past decade
or so? If so why?
A: The most important reason is our aging population (late 70s
for males and over 80 for women..) Due to living longer, it follows that
more Lankans are now at risk of AD with advancing age. Improved
awareness of the disease among the public and medical fraternity has
also contributed to increased detection of patients and increased
reporting.
Q: Dementia and Alzheimer's - are they the same thing?
|

Apathy and depression are early symptoms |
A: Dementia is a group of symptoms characterized by a decline
in intellectual functioning severe enough to interfere with a person's
normal daily activities and social relationships. There are different
types of Dementia, and Alzheimer's disease is the most common type of
dementia in older people.
Q: What are the main causes for Alzheimer's?
A: Most experts believe that the majority of Alzheimer's disease
occurs as a result of complex interactions among genes and other risk
factors. Age, family history and heredity are all risk factors we can't
change. Now, research is beginning to reveal clues about other risk
factors we may be able to influence through general lifestyle and
wellness choices and effective management of other health conditions.
Growing evidence links brain health to heart health.
The risk of developing Alzheimer's or vascular dementia also appears
to increase when certain pre-conditions damage the heart or blood
vessels, such as, high blood pressure, heart disease, stroke, diabetes
and high cholesterol. Studies have found an association between lifelong
involvement in mentally and socially stimulating activities and reduced
risk of Alzheimer's disease. These include higher levels of formal
education, a stimulating job, mentally challenging leisure activities,
such as reading, playing games or playing a musical instrument and
frequent social interactions.
Q: Who are most at risk of Alzheimer's?
A: The likelihood of developing Alzheimer's doubles about
every five years after age 65. After the age of 85, the risk reaches
nearly 50 percent. People with rare genetic changes may develop
Alzheimer's symptoms as early as in their 30s.
Q: Symptoms to look for?
A. A common symptom is memory loss, especially, forgetting
recently learned information. Others include forgetting important dates
or events and asking for the same information repeatedly. Some people
may experience changes in their ability to develop and follow a plan
(e.g. a recipe) or work with numbers (e.g. bills). Apathy and depression
are also often early symptoms. Late symptoms include impaired
communication, poor judgment, disorientation, confusion, behavioural
changes and difficulty in speaking, swallowing and walking.
Q: How early do they present?
A: Pathological changes in the brain probably start 10-20
years before any visible signs or symptoms of the disease appear. Memory
loss, the first visible sign, is the main feature of mild cognitive
impairment (MCI).
Q: Is it curable? Can AD be treated?
 A: Currently there is no cure for Alzheimer's disease.
However, some drugs may help delay the progression of symptoms
associated with the disease. Also, some medicines may help control
behavioural symptoms, such as sleeplessness, agitation, wandering,
anxiety, and depression. Treating these behavioural symptoms often makes
people with Alzheimer's more comfortable and makes their care easier. A: Currently there is no cure for Alzheimer's disease.
However, some drugs may help delay the progression of symptoms
associated with the disease. Also, some medicines may help control
behavioural symptoms, such as sleeplessness, agitation, wandering,
anxiety, and depression. Treating these behavioural symptoms often makes
people with Alzheimer's more comfortable and makes their care easier.
Q: What is the treatment procedure in Sri Lanka?
A: The first step in the process is to diagnose AD. There is
no single test that can show whether a person has AD or not. While
doctors can almost always determine if a person has dementia, it may be
difficult to determine the exact cause. Diagnosing Alzheimer's requires
careful medical evaluation and tests (such as blood tests and brain
imaging) to rule out other causes of dementia-like symptoms.
Among drugs recommended for treatment in AD, only two drugs are
available in Sri Lanka. These drugs are recommended only for mild to
moderate disease.
Q: What are the benefits of such treatment?
A: As AD progresses, brain cells die and connections among
cells are lost, causing symptoms to worsen. While current medications
cannot stop the damage AD causes to brain cells, they may help lessen or
stabilize symptoms for a limited time by affecting certain chemicals
involved in carrying messages among the brain's nerve cells.
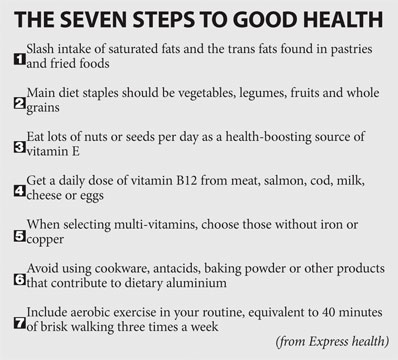
Q: Can certain foods delay onset of Alzheimer's?
A. Strongest evidence for antioxidant protection against
Alzheimer's disease rests with high food intake of vitamin E. The
richest food sources of vitamin E include vegetable oils, margarine,
nuts (especially almonds), and seeds (especially sunflower seeds).
Moderate amounts of vitamin E are found in whole grains, egg yolk,
and a limited number of vegetables (eg, cabbage, broccoli) and fruits (eg,
avocados, apples, melon).
Q: Is there a genetic link to Alzheimer's?
A: Over 95% of patients have sporadic AD (without a family
history and onset after 65 years) and their family members are not at
increased risk of developing AD. The most common gene associated with
late-onset Alzheimer's disease is called apolipoprotein E (APOE).
The presence of this gene increases the risk of AD but does not cause
AD. About 5% of patients with AD have familial Alzheimer's disease,
which is an early-onset form of the disease that appears to be
inherited. In familial Alzheimer's disease, several members of the same
generation in a family are often affected.
A: What part of the brain is most vulnerable?
A: Alzheimer's disease damages and kills brain cells. Early in
the disease, destruction of neurons is particularly widespread in parts
of the brain that control memory, especially the hippocampus.
The other part of the brain that sustains major damage is the
cerebral cortex, particularly the areas responsible for language,
reasoning, perception, and judgment (the temporal, frontal, and parietal
lobes).
Q: What are the new breakthroughs or advances in Alzheimer's
in recent years?
A: Several clinical trials of investigational drugs targeting
the disease process are under way. In addition to investigating these
experimental drugs, many clinical trials are in progress to find various
brain imaging studies and testing of blood or spinal fluid for a
biomarker to diagnose Alzheimer's Disease in its earliest, most
treatable stages - possibly, even before symptoms appear.
Several professional organizations have published updated guidelines
on the management of AD and are available for use locally.
Q: What are the gaps in treating Alzheimer patients in Sri
Lanka?
A: Patients with AD should be managed by a multidisciplinary
team including neurologists, psychiatrists, neuropsychologists,
specialist nurses, occupational therapists, social workers and care
givers. Non-availability of new drugs and the treatment cost, are some
shortcomings. From a diagnostic and monitoring point of view, lack of
neuro psychologists in the country is a major problem in managing
patients with AD. Patients' own family members or relatives are the main
care givers in Sri Lankan society.
At present, the biggest burden on the health sector is from diseases
affecting the elderly. Of this, stroke and dementia (of which 60% is
Alzheimer's) are the commonest, and impose a major burden on family
members as care givers.
Q: Does your hospital have any plans to meet these challenges?
Does the Health Ministry?
A: The emerging threat of health issues concerning a rising
elderly population has been foreseen by the Health Authorities in many
countries including the Ministry of Health in Sri Lanka.
Strategies are already under way to meet this threat in terms of both
prevention and care, but a lot more needs to be done. Non-communicable
diseases (NCD) unit of the Ministry has set up island wide NCD
prevention clinics through surveillance. Finally, I wish to stress that
Geriatrics (Care of the Elderly) needs to be more widely recognized as a
medical sub specialty and the fact that a diploma program in this
direction has already been launched by the Postgraduate Institute of
Medicine PGIM is a step forward. Hospitals also need to have special
clinics for Elderly Care such as the one now operating at the Sri
Jayewardenepura General Hospital. |







