|
 |
| Sunday, 14 September 2003 |
| Features |
| News Business Features Editorial
|
Fever and laboratory diagnosis Fever is not a disease, it is a symptom of a disease. There are three classical types of fever: a) Continued fever, b) Remittent fever and c) Intermittent fever. When the fever does not fluctuate more than about 1 degrees C (or 1.5 degrees F) during the twenty four hours, but at no time touches the normal (37.2 degrees C - 98.4 degrees F) it is described as continued. When the daily fluctuations exceed 2 degrees C it is known as remittent and when fever is present only for several hours during the day it is called intermittent when a paroxysm of intermittent fever occurs daily the type is called quotidian type fever. When it occurs on alternate days it is known as tertian type. When two days intervene between consecutive attacks it is referred to as quarital type. However with the use of antibiotics and other specific drugs these classical types of fever are not often seen.
When a patient comes to a physician he has to diagnose whether it is due to bacterial infection or viral infection. In a bacterial infection a simple blood count shows increase leucocytes with a high percentage of neutrophils. If it is a viral fever there will be a low white cell count. To diagnose dengue labourtory investigations are very vital. It is transmitted to man by mosquitoes chiefly "Aedes aegypti" the platelet count is important to diagnose. In dengue fever the platelet count will go down to 20,000 per cu mm cent normal range over 150,000 per cu mm. Mild dengue fever may resemble other viral diseases and a severe attack may be mistaken for anicteric yellow fever. But the absence of urinary changes will help to differentiate it. Blood for dengue antibody litres will confirm it. Another common fever is Malaria fever. Blood film stained by leishman stain or giemsa stain can identify the Malaria parasites, plasmodium vivax or p. malaria. Similarly filarial infection also can give fever symptoms. Blood film for Micro filaria or a Filarial antibody test, or increase eosinophilic count can confirm it. Salmonellae infection can also cause fever. Salmonellae can cause a number of different conditions, namely Typhoid and Paratyphoid fevers. Blood count, blood for S.A.T. (Standard Agglutination Test) can confirm Typhoid fever. A specimen of the patient's stool or vomit together with the suspected food if available should be sent for culture. Tuberculosis also gives a symptom of fever, blood for E.S.R. (Erythrocyte Sedimentator Rate) will increase to about 50 mm in 1st hour Tubercle Bacilli can be isolated in sputum for A.F.B. Test (Acid Fast Bacilli) smear is stained with ziehl neeson stain (2.n. stain). Sputum for T.B. culture is also important. The isolation of tubercle bacilli is absolute proof of the diagnosis. Urine infection is another indication, when a patient with fever comes to the physician he should request a urine full report and culture with ABST. If there are pus cells, red cells in the urine that indicate urine infection, culture will confirm the bacteria which cause infection. Then the diagnosis and treatment is simple. Viral infection is now the commonest cause of Meningitis. Bacterial Infection and tuberculosis meningitis is also seen. Meningitis is the inflammation of the meninges, high fever is a main symptom. Full Blood Report, C.S.F. (ceribro spinal fluid) Full Report and Culture will help for early diagnosis. C.S.F. may be turbid as there is an excess of lymphocytes C.S.F. report will show an excess of polymorph nuclear leucocytes and the causative organism can be isolated. We can see high intermittent fever during leishmaniasis diagnosis is established by demonstrating the parasite in stained smears of aspirates of bone marrow, lymphrode spleen or liver. A well managed laboratory will help the physician to diagnose many diseases with early symptom of fever. - A.D.T. Maithripala, Medical Lab Technologist ############# 1. Plasmodium vivax. Ring stage. x 2000 2. Plasmodium vivax. Amoeboid form. x 2000 3. Plasmodium vivax. Fully developed schizont x 2000 4. Plasmodium vivax. Male gametocyte. x 2000 5. Plasmodium vivax. Female gametocyte. x 2000 6. Plasmodium malariae. 'Compact' form x 2000 7. Plasmodium malariae. 'Band' form. x 2000 8. Plasmodium malariae. Fully developed schizont. x 2000 9. Plasmodium ovale. Female gametocyte. x 2000 10.Plasmodium ovale. Fully developed schizont. x 2000 11.Plasmodium falciparum. Red blood corpuscles containing various types of young ring. x 2000 12.Plasmodium falciparum. 'Old' ring, showing altered staining reaction and Maurer's dots. x 2000 13.Plasmodium falciparum. Male gametocyte or crescent. x 2000 14.Plasmodium falciparum. Female gametocyte or crescent. x 2000 15.Plasmodium falciparum. Pigment in polymorphonuclear leucocyte. x 2000 16.Leishmania donovani from a spleen smear. Some lying free and others within the cytoplasm of an endothelial cell. x 2000 17.Trypanosoma cruzi. Adult form as seen occasionally in the blood of patients suffering from Chagas' disease. x 2000 18.Borrelia recurrentis. x 2000 19.Filaria loa. x 600 20.Trypanosoma rhodesiense as seen in a thick blood film of patients suffering from trypanosomiasis. x 1000 ############ EPA's cancer guidelines for children Smoking and musculoskeletal - related disability A recent study has shown how cigarette smoking can affect development of physical disability following initial musculoskeletal - related hospitalisation. Researchers in Washington DC, USA followed 15,140 US Army personnel hospitalised for common musculoskeletal disorders between 1989-1996 for up to 8 years (1997) to assess risk for long-term physical disability. Trends between increased smoking level and long-term disability were identified for persons with knee injuries, rotator cuff injuries, and intervertebral disc displacement. In proportional hazards models, disability was significantly associated with heavy smoking among all subjects. Both heavy smokers and light to moderate smokers were at greater risk for disability following meniscal injuries. Excess fraction due to smoking among subjects with meniscal injuries who currently smoke was 38 percent. Lincoln AE et al. The effect of cigarette smoking on musculoskeletal-related disability. AM J Ind Med 2003 Apr, 43 (4): 337-49. Smoking and risk of haemorrhagic stroke Smoking is an established risk factor for ischemic stroke and subarachnoid haemorrhage (SAH), but the impact of smoking on intracerebral haemorrhage (ICH) is less clear. In a prospective cohort study among 22,022 US male physicians participating in the Physicians' Health Study, incidence of stroke was measured by self-report and confirmed by medical record review. This prospective study suggests an increased risk of total haemorrhagic stroke, ICH, and SAH in current cigarette smokers with a graded increase in risk that depended on how many cigarettes were smoked. The effect of smoking on ICH is of about the same magnitude as the effect of smoking on ischaemic stroke. The results add to the multiple health benefits that can be accrued by abstaining from cigarettes smoking. Courtesy: IATH Bulletin ########### Do you need to... Change your bowel habits?
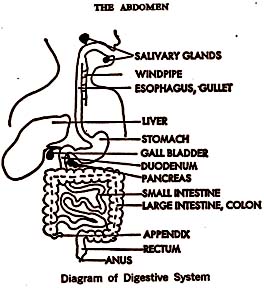
People's bowel habits are the result of environmental influence as well as what goes on inside the body. Elimination is a private, personal affair and is a highly complex action. Consequently, something can go wrong at any one of many stages to block or change the end result. Therefore, when considering a problem of change in elimination we must look outside as well as inside for the cause. If we examine our day's activities we find that we do not follow the same routine every day. We do not eat the same amount or variety of food each day, nor are we entirely regular as to mealtime. Therefore, our bowel function varies from day to day. It is not unusual to note that when you are on vacation your bowels move much more regularly and in a more satisfactory way than when you are at home. You may blame the change on the fact that you are drinking different water. In reality, water has nothing to do with it. The change is in emotional tension, relieved by lessened responsibility. It is impossible to define what is exactly normal, for everybody is an individual unto himself and no two people are alike. This rule applies to everything about human beings. There is no exact pattern for anything. There are two major divisions of the intestinal tract - the small intestine and the large intestine, or colon. The first is devoted to the process of digestion and absorption of foodstuffs. What is wanted by the body is taken into the blood stream and what is rejected remains and is carried to the colon. This material reaches the right side of the colon (the caecum) in a liquid state and is retained there for a time. As it begins to move along, fluid is removed gradually and the mass begins to solidify, until it reaches the descending colon and sigmoid flexure on the left side, where it becomes more or less solid. It is stored there until the time comes to expel it from the body. When a normal stool is evacuated it is an inch or an inch and a half in diameter and in sections eight inches in length. It is made up of about two-thirds waste material and one-third bacteria, many of which are dead. The waste material is partly food that was not absorbed and partly material that was discharged into the bowel from the blood stream. The bacteria are harmless when in the colon, but some of them could cause trouble if they were to break through normal body defences and get into the blood stream. There are many different kinds of bacteria. To some extent their relative numbers depend on the diet the person eats. The so-called colon group of bacteria are preponderant when a diet high in meat, fish and egg protein is eaten. The lactobacillus thrives on a high carbohydrate diet with lots of sugar and starch. It is said that eating a lot of yogurt encourages the bacillus acidophilus to grow. This bacillus is supposed to have a beneficial effect, particularly as to length of life. Normally mucus is present in the colon and in small amounts in the stool. It acts as a protective covering of the colon lining. If it was not there we would not live long. Occasionally there is an excess in the bowel movement, which appears slimy. As a rule it means little or nothing - certainly no indication of a diseased condition. There is nothing really "dirty" about either the colon or its contents. As a rule the consistency of a bowel movement is uniform, but occasionally there may be vegetable fibres and even undigested food. After corn on the cob has been eaten it is not at all unusual to see whole kernels. This appearance means that the person did not chew thoroughly. The coarser leafy vegetables eaten too rapidly and in large quantities may appear unchanged. The person who has no acid in his stomach consistently sees fibrous material. In an older person it may be normal to have no such acid, or it may mean something fairly serious, having to do with poor absorption of foods. Odour The type of food has a great deal to do with the odour. A high proportion of meats and eggs in the diet produces a typical smell due to hydrogen sulphide. A large amount of fish, particularly of the oily varieties, produces an even more odoriferous bowel movement. If the stools are consistently foul smelling for a considerable time, there may be a serious digestive disturbance, and the person should see his doctor. The stools of people who live on a vegetarian diet have little or no smell, and those of people consuming only milk have no smell at all. Diet makes the difference. The normal colour of the bowel movement is brown. This effect is produced by pigment in the bile, which is a digestive juice secreted by the liver and delivered into the small intestine by way of the gall-bladder. The colour may be consistently dark brown or greenish and still be normal. If there is much milk in the diet it may be light yellow, like that of a baby. Again the difference is in the diet. Beware of the black stool of tarry consistency. It means partly digested blood from the region of the stomach. If you should notice your stools to be like this, first be sure you are not dealing with a dark green colour. Look at a specimen in daylight. The consistency is sticky or tarry. Usually such a stool appears suddenly, and there are symptoms of blood loss. It is not the sort of thing that goes on week in and week out. Red blood comes from the lower end of the intestinal tract. Usually it is on the outside of the stool in streaks or it may follow after. Although statistically this blood is probably not of serious import, it is one of the signals of early cancer, and should be looked into right away. Do not wait to see whether it recurs. The object in curing cancer is to diagnose early. See your doctor immediately. The clay-or putty-coloured stool means that there is no bile getting into the intestinal tract from the liver. Along with this symptom the urine is dark in colour and the skin is yellow if you look closely in daylight. The whites of the eyes are easier to adjudge, particularly if the skin is dark to begin with. Go see your doctor, or - better - get him to see you, for a "touch of jaundice" may well be serious. The stool can be hard, lumpy, soft, broken up, and pasty, and the person still be in good health. If it appears oily and greasy there may well be excess fat, which means an absorption problem. A brief attack of diarrhoea once in a great while probably means nothing particularly except that the person caught some sort of germ. However, if he has liquid bowel movements day in and day out, especially if there is some abdominal cramping and a little blood, this condition is a must for seeing his doctor. No one can say exactly how many bowel movements you should have during a day if you are healthy. This situation depends on many factors. There are people who have had three or four a day for years and lived to a ripe old age. There are other people who have had only one every second or third day and remained healthy. The main thing to keep in mind is that a change in habit may be significant. If the person has always been on the difficult-to-move side and then develops frequency, or vice versa, he should seriously look into the matter. From Herald of Health. |
|
News | Business | Features
| Editorial | Security Produced by Lake House |