|
 |
| Sunday, 18 April 2004 |
| Features |
| News Business Features Editorial
|
Probing the wall of silence...
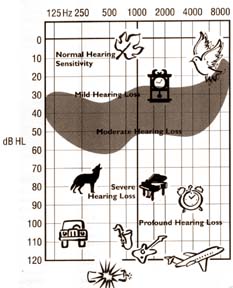
Hearing impairment is the second most common disability next to loss of vision. A. M. R. L. ATTANAYAKE, an experienced Hearing Audiologist explains to CAROL ALOYSIUS how hearing defects can be detected at an early stage, and how they can be overcome. Q: What are some of the causes for hearing defects? A: Causes vary from age related degeneration processes that result in especially high frequency losses, to exposure to loud noises such as the train, buses, cars (this is one reason why engine drivers and bus drivers develop hearing defects by their mid 50s); from congenital defects such as children from a marriage between two blood relatives, to Rubella, hyperbiliruenia (jaundice). From meningitis, fits, hyperroxia, premature birth, trauma and head injuries. Other causes include middle ear infections, perforation in the ear drum, eustachian tube dysfunction, ototoxic drugs (used for high blood pressure, diabetes and a high dosage of life saving drugs. Wax in the ears, sudden shock and sudden loud noise are other causes. Q: How do you classify hearing losses? A: Hearing losses can be classified into (a) Conductive losses i.e. problems in conduction due to wax, middle ear dysfunction, Eustachian tube dysfunction or perforation in the ear drum caused by cotton buds used to clean the ear or loud noises. (b) Sensory neural losses. This is due to either cochlear or retro-cochlear pathologies or cranial nerve problems. Both these conditions are incurable and lead to permanent hearing losses. Q: What is the normal decibel hearing scale? A: Between 20 plus or minus DBHL (Decibel Hearing Level Scale). The loudest is around 140. It can also vary in between these scales. Q: How does one know if a very young child has a hearing defect? A: If the child doesn't respond to normal conversational sound and shows no noticeable response to sounds in other intensities, consult an ENT doctor. Q: What kind of tests are done to evaluate a child's hearing at a early stage?.. A: Tests depend on the child's age:
Reinforcement test. Here if the child can keep his back straight we do play audiometry, by putting a head phone on the child and making a sound that will force the child to turn his head in that particular direction. If the child can't keep his back straight we use a rattle or some other toy to make sounds. Free field testing. Here sounds are given at certain distances and we watch the child for his reactions. Sometimes he may hear boom based sounds i.e. rough voices coming from low frequency and not the phone ringing or vice versa. This could mean the child has a low or high frequency hearing loss. Q: Any other tests? A: We have subjective tests and objective tests. The former are done directly with the child. The other tests are done with or without the child's co-operation. e.g. the Middle Ear test is done without the co-operation of the child by using a scale derived from the mass and stiffness of the ear to obtain certain information. Another test called the ABR (Auditory Brainstem Responses) are used to test the outer ear to auditory cortex. This is a nerve conduction test but by using selected frequency band stimulus you can get a frequency specific valve of hearing of the subject. The third is the Auto Accoustics Emission. Here, by collecting the cochlear microphonic produced by the outer hair cells in the cochlear and the oval window, we can get some form of hearing. If the loss is due to degeneration of nerve cells in the cochlear, it is called cochlear loss or sensory loss. Q: What happens when someone is exposed to a loud noise? A: It could result in sensory nerve losses. Loud music and the continued use of walkmans can lead to a condition called Tinnitus. If you are exposed to some loud noises for a short period you can get temporary hearing loss which is called Temporary Threshold Shift. If exposed to loud sounds for longer durations, you can develop permanent hearing losses. This is called Permanent Threshold Shifts or noise induced hearing problems. Q: Are there any other hearing complications resulting from loud noises? A: You may start hearing ringing and hissing sounds or whistling sounds in the ear. This condition is called Tinnitus as I mentioned earlier. This can last for some time requiring Tinnitus re-training therapy or group counselling which might help to eliminate unnecessary fears or phobias. Q: Tell us about the various hearing aids available for those with hearing defects. A: Hearing aids use two systems; Analogue and Digital. By using a digital p.c. you can program the analogue system. Q: Explain. A: The analogue system amplifies sounds and does not modulate or process. To modify sounds you can simply cut off some sounds or emphasise some sounds up to a limit. But this will not mimic cochlear function or the process. Digital hearing aids only process sound using averaging systems in a linear and un-linear way that can to some extent mimic the cochlear function. Q: Can a patient wear a hearing aid straightaway without being trained to use it? A: Patients using hearing aids must undergo some accoustic or auditory training to get acclimatised. Acclimatization is a very slow process for which the patient needs a good support system from his doctor, speech therapist, audiologist, parents. Q: Is the sound you hear from a hearing aid similar to normal sound? A: The way you hear from a hearing aid is completely different from the way you hear even with impaired hearing. So it takes some time to get your auditory pathways and the senses in the brain trained (acclimatised). Q: What advice do you have for patients requiring hearing aids.? A: There are three golden Ps they must follow; Patience, Practice and Perverence. The best way to learn how to use a hearing aid is to speak as much as you can and hear your own voice. ############### Restless legs It has been a long day and you are exhausted. You crawl into bed, longing for sleep, but your limbs have other ideas. Within moments, you experience a burning sensation in your calves, accompanied by an uncontrollable urge to move your legs. Kicking brings relief, but not for long. If you recognise these symptoms, you may well be among the many people who suffer from restless legs. The cause of restless legs, also known as Ekbomsyndrome, has not been identified but it may be linked to a lack of dopamine in one of the brain's receptors, which affects the spinal cord reflexes. Studies at Penn State College of Medicine in Chicago confirmed that iron deficiency in the brian also plays a part. Dr. K. Ray Chaudhuri, one of the few British experts on Ekbom syndrome, believes the condition has a huge psychosocial impact. "Chronic sleep deprivation over a period of eight to 10 years - which is how long it takes on average to get a referral to a specialist - can affect cognition, raise anxiety levels and impair daytime functioning." Some doctors believe the problem is psychosomatic or mis-diagnose it as night cramps. Treatment for cramp is useless, and sleeping tablets can actually make it worse. Walking and stretching, taking a bath, relaxation exercises, massaging the limbs or resting the feet on a cold surface may help. If a blood test reveals low iron levels, taking iron supplements can stop the attacks. New drugs are under development. Telegraph Group Limited. ############### Dark circles under the eyes Lifestyle, heredity, aging and illness can all contribute to dark circles under the eyes. Tiny blood vessels close to the surface (thin skin) and excess melanin pigment in the skin (hyperpigmentation) both darken the skin itself. Bulging lower eyelids can also cast shadows. Tips for decreasing under-eye puffiness: Prevention: Be sensible about sun exposure, don't smoke, get enough sleep, eat right, and drink plenty of water * Sleep with your head slightly elevated to reduce fluid retention * Avoid alcohol and salty foods, which promote tissue fluid retention * Take antihistamines if you have allergies; don't rub your eyes * Use caution when removing makeup to avoid getting any in your eyes * Use a moisturizer to avoid dryness that can lead to irritation and swelling * Cooling the eyelids with wet tea bags or slices of curumber may temporarily reduce puffiness * There does not appear to be any truth to the rumor that Preparation H reduces dark circles There are also medical approaches available. Bleaching creams or special light treatments may help lighten skin. Chemical peeling removes the top layer of skin, eliminating fine wrinkles, and may also lighten hyperpigmented skin. Surgery to reduce the fat pad in the lower eyelid may decrease the shadowing effect. One type of laser can be used to remove the surface skin, much like a chemical peel. Another type is used to destroy highly pigmented cells without harming other tissue, much the same way tattoos are removed. (United Feature Syndicate) ############### Obesity in childhood by Dr. D.P. Atukorale Many parents in Sri Lanka don't consult their paediatricians or dietician when they have obese children. Some Sri Lankans have the misconception that obesity in childhood is a sign of good health and so they never take these obese children to paediatricians for advice. Thus very obese children in Sri Lanka don't get the appropriate treatment. The rise in the prevalence of childhood obesity in U.K. has been appropriately labelled as an epidemic and the adverse consequences of childhood obesity are increasingly recognized. It is common knowledge that childhood obesity persists into adult life. Obesity in children is different from obesity in adults. The most obvious difference is that children and adolescents need to grow during puberty; adolescents will double their weight and increase their height by 20 per cent. In adults, obesity is expressed as body mass index (BMI, weight in kilograms divided by height in metres squared) In adults a BMI of 26-30 Kg/m2 is considered overweight, BMI of 30-40 is considered obese, and BMI greater than 40 is considered morbid obesity. But in children such a simple expression of obesity unrelated to age, sex or ethnic background is not possible. In obese children over enthusiastic management of obesity may result in restriction of dietary energy and would compromise normal growth and development. Unlike treatment of adult obesity, weight maintenance is often a suitable goal in childhood. Clinical nutrition assessment in childhood and adolescence revolve around energy (food) intake minus energy output (resting metabolic rate plus activity). In contrast to adult life where energy balance should be zero, children need a small continuing positive energy balance to support normal growth. An excess continuing positive balance will lead to excess stores of energy and thus obesity. It is not only fat which accumulates but also excess of lean body mass. The sources of chronic energy-positive balance leading to obesity are increased energy (food) intake and reduced energy expenditure by either lack of physical activity or an increase in sedentary behaviour. The simple energy balance equation is poorly understood by some of the parents of these obese children who often believe that their children have metabolic problems. Childhood obesity is becoming more and more common in the higher socio-economic groups especially in the urban areas of Sri Lanka. As far as I am aware, there are no statistics regarding prevalence of obesity in childhood and adolescence in Sri Lanka. One cause of childhood obesity is due to more food eaten away from home. Another cause of childhood obesity is lack of physical activity. Does childhood obesity matter? The most common side-effect of childhood obesity is psychological morbidity. In obese children there is an increase in a cluster of cardiovascular risk factors such as hyperlipidaemia, high blood pressure and abnormalities in left ventricular mass, hyperinsulinaemia and prevalence of type II diabetes. There is a link between childhood obesity and bronchial asthma and rarer complications are orthopaedic problems and development of fatty liver. The consequences of childhood obesity for adult life are persistence of obesity, significant increase in cardiovascular risk factors, socio-economic effects and long term morbidity and mortality. Prevention There is no evidence at all that drug therapy or surgery is of any help in these obese children. There should be reduction in sedentary behaviour, increase in life style physical activity dietary approach and family involvement. There is also evidence to show that childhood obesity is a social problem rather than one that we can expect individual children and their parents to solve. ############### Raising healthy kids Studies have shown that children who eat breakfast do better at school, pay better attention in class and are less likely to have behaviourial problems. Eating breakfast also help children to meet their daily nutritional needs and avoid weight problems. No time to cook breakfast in the morning ? Here are some time-saving solutions: Stock up on low-fat granola, or fruit that children can eat on the way to school. A bowl of breakfast cereal and milk takes very little time to prepare and is a nutritious way to start the day or try cereal drinks that can be consumed after leaving the home. If your children are resistant at meal times or insisting on less healthy options, try these suggestions for meal-time peace: Encourage them to help out in meal preparation. Studies and parental experience show that children are more likely to eat something they helped prepare. Having the kids help out may be more troublesome in the beginning but in the longer term would actually cut food preparation time with your new kitchen "helpers". Make sure kids don't snack too close to meal times. Be realistic about children's food portions and hunger levels. Forcing children to clean up their plates even when they are not hungry may lead to a life-time of weight problems. Ban TV-watching during meal times. This encourages children to concentrate on their food and enjoy their meal more and ultimately be more attuned to when they are full. Veggie Power Nutritionists recommend that the daily diet should consist of at least five servings of fruits and vegetables. Let your children select the fruits and vegetables they want to eat. Hide the vegetables e.g. add carrots, tomatoes, ladies fingers/okra and other vegetables in curries, stews, pasta sauces, omelettes, etc, or order up extra vegetables as pizza toppings. Put lots of salad such as, cucumber, lettuce and tomatoes in sandwiches. Snack Smart Snacking can be a healthy way for children to get sufficient energy and nutrients throughout the day. There is also emerging evidence that regular sensible snacking in response to feeling 'peckish' helps prevent weight gain, probably by staving off binge-eating in response to ravenous hunger. However not all snack are created equal. Stock up the house with easy to eat fruits like bananas, apples and waxs apples (jambu merah). Buy pre-cut fruits at the supermarket. Keep dried fruit, roasted nuts, whole-wheat biscuits, cheese slices and yoghurt for at-hand and ready-to-eat for children to snack on. From Food Facts |
|
News | Business | Features
| Editorial | Security Produced by Lake House |