 |
  |
| Sunday, 19 September 2004 |
| Features |
| News Business Features Editorial
|
World Alzheimer's Day on Sept. 21 : High dietary cholesterol and dementia By Dr D. P. Atukorale Dementia consists of progressive intellectual deterioration leading to loss of memory and mental ability as a result of brain damage. There are a large number of causes of dementia, ALZHEIMERS disease being the most common. Our process of knowing namely cognitive function includes both awareness and judgement. There is scientific evidence that dietary factors influence our cognitive function and subsequently the risk of dementia. Antioxidant intake is associated with lower risk of dementia whereas saturated fat and high cholesterol intake were found to be associated with higher risk of dementia. Some recent studies have shown evidence of a protective effect of cholesterol lowering drugs such as statins in dementia Moderate fish consumption and omega 3 fatty acids (PUFA) in take was related to reduced risk of dementia in particular. Alzheimers disease may be attributed to several mechanisms such as anti-inflammatory effect of omega 3 PUFA, a decrease in risk of Cardiovascular Disease or an increase in the neuroplasticity of nerve membranes. Sub-clinical phase of declining in cognitive function precedes Alzheimers Disease by decades. A population based study involving 1613 men and women whose age ranged from 45-70 years showed that fatty fish and marine omega - 3 PUFA consumption was associated with a reduced risk of cognitive performance and intake of cholesterol and saturated fat was associated with an increased risk of impaired cognitive function in middle aged population. In animals high cholesterol diet leads to accumulation of Beta amyloid in the brain which subsequently leads to the formation of amyloid plaques that is pathognonomic of Alzheimers Disease. Dementia is a very common disease in the West. In UK 8 per cent of all people over the age of 65 suffer from dementia which is a disorder of late life. It is estimated that there are 18 million people suffering from dementia world wide. As far as I am aware there are no statistics regarding prevalence of dementia among Sri Lankans. There is a definite relationship between consumption of saturated fat (e.g. red meat) and Heart Disease. But very few readers are aware about the fact that excessive consumption of cholesterol and saturated fat causes deterioration in cognitive function which subsequently leads to dementia. Therefore it is advisable to restrict the consumption of food items such as red meat (which contain large amounts of saturated fatty acids) and eggs, prawns, crabs and lobsters which contain very high concentrations of cholesterol with a view to prevent deterioration in cognitive function and dementia. ****** NO TIME TO LOSE Alzheimer awareness building commenced just twenty years ago at the formal inauguration of Alzheimer's Disease International. During the intervening years, 67 countries, including Sri Lanka pledged their support. Dementia causes slow brain death. Initially, confusion occurs when recent events cannot be converted to reliable memories. Cognitive decline in old age is expected, but the mild forgetting in the senior years is a far cry from dementia. Gradual removal of memory capacity is a form of slow death; 8-20 years later the second death of the body occurs. In Sri Lanka there is scant knowledge of the complexities of dementia, from early diagnosis to the progression of the disorder and the commitment needed to provide 24-hour care in the latter stages, when those stricken are hundred percent dependent. The reality of the terrible effect of dementia on family and the community are generally not visible due to ignorance and stigma. The American Alzheimer's Association, which has recently acknowledged the capacity of dementia to be an awesome epidemic in the next 40 years, has adopted the slogan, 'Save the Brain' with an emphasis on brain health through appropriate nutrition, correct lifestyle, positive thinking and continuing engagement. The Alzheimer's Disease International will ask all of its constituent members, at the 20th Anniversary World Conference, which will be held in Kyoto - October 2004, to adopt the slogan 'No Time to Lose'. The expectation is that the current estimated world figure of 18 million afflicted persons, will rise to 36 million or more in the next three to four decades. Today, there are 600 million people in the world aged 60 years and over. This figure is expected to double by 2025 and to reach two billion by 2050, the vast majority in the developing world. Population ageing is characteristically accompanied by an increase in the burden of chronic noncommunicable diseases (NCDs) such as Cardiovascular Diseases, Diabetes, Alzheimer's Disease and other ageing-associated mental health conditions, cancers, chronic Obstructive Pulmonary Disease and musculoskeletal problems. As a consequence, pressure on health systems worldwide will increase. **************** When two 'thal.minor' persons marry...
Q. What exactly is Thalassaemia? A. We have a Pigmented Protein in our red cells called haemoglobin which carries oxygen. In Thalassaemia the production of this protein is reduced which in turn results in the reduction of the oxygen carrying capacity. Q. How does one get this disease? A. When two Thalassaemia minor (thal.minor) patients marry and have children. Q. Are all children born out of such a marriage at risk of this disease? A. Let me put it this way. If two Thalassaemia minor patients get married and have children, there is a 25 per cent chance of them having a Thalassaemia major (the more severe form of the disease) baby, and a 50 per cent chance of having a Thalassaemia minor baby. Q. What kind of treatment is available for a child who is born with Thalassaemia major? A. In the case of Thalassaemia major patients, the only treatment we have for them in Sri Lanka is to give them someone else's blood which is compatible with theirs. This must be done on a regular basis for the rest of their lives. Q. Can this have an adverse effect on their health? A. Giving blood on a regular basis to these patients can lead to the risk of infections and adverse reactions because transfusions are not hundred per cent risk-free even though the blood we give is well screened. It is also a strain on the blood bank. They can also suffer from excess iron which causes tissue damage. Thalassaemia major patients can also get severe anaemia, jaundice, and suffer from retarded growth and recurrent infections. Many of them rarely survive beyond the age of 30 years because of iron toxicity, or some intercurrent infection and recurring anaemia. Q. You referred to Thalassaemia minor patients. Do they require the same treatment? A. No. Thalassaemia minor patients can lead a normal life as they are not seriously affected by the disease. Overall, their haemoglobin level is in the range of 9-11 gram/dL, so they don't need blood transfusions. They may thus be not even aware of their condition until it is detected 'accidentally'. Q. How? A. When their condition is compounded by some other anaemia e.g iron deficiency, or any other anaemia. Q. How is the condition detected? A. Detection is by laboratory diagnosis as the patient will not have any clinical symptoms. So when the blood is sent for a lab test, the haematologist will be able to detect and confirm the diagnosis with a test called HbA2. Q. Do patients with Thalassaemia minor have any symptoms at all that can indicate this 'hidden' condition? A. The first clue to having thalassaemia, as I said, is anaemia, the symptoms of which are fatigue and lethargy. Unfortunately, most Thalassaemia minor patients don't come with these presentations and it is only when they come for a routine blood test before some surgery, that the condition is detected. Or else if their condition is compounded by some other cause for anaemia, or during pregnancy. This is why it is so important to prevent the condition in the first place. Q. As haematologists you play a very important role in detecting the Disease. I understand that you are also preparing for an awareness campaign to prevent the spread of Thalassaemia. Can you explain how you will be doing this? A. Haematologists are the front line doctors who detect the Disease when a blood sample is sent to a laboratory. So we are in a position to educate and advise people about the Disease. As I mentioned before, the only way you can prevent it is by preventing the marriage of two thalassaemia minor patients. If a Thalassaemia minor patient marries a normal person there will be no risk of giving birth to a thalassaemia major baby. Q. Upto now the concentration has been on how to manage these patients. I understand that your college is to launch a new campaign to prevent the disease. Tell us about it. A. Our campaign will be concentrating on prevention not only because Thalassaemia is easily preventable, but because the treatment of Thalassaemia patients is so costly. Over 5 per cent of the health budget is spent on management of these patients whose lifespan is limited. Q. What do you see as the need of the hour in respect of this disease? A. We need more haematologists in the hospitals to begin with. Ideally there should be haematologists in all provincial teaching hospitals, but because of the dearth of doctors many hospitals have no haematologists on their staff. We also need accurate interpretation of tests e.g., high quality blood pictures, automated red cell indices and HbA2 analysis both in the government and private sector. This is the responsibility of the haematologist who has been trained for these tasks and have the skills to deliver the goods. We also have to ensure accurate diagnosis of these patients, for which again haematologists in this country have the training. Q. Would you say that preventing and managing Thalassaemia requires a team effort? A. Certainly. We should use the haematologists in the university and doctors in the health ministry to form this team. We need the services of paediatricians to manage the Disease, haematologists, blood transfusion specialists, nurses, as well as the co-operation of social service organisations. All these people are needed to make up a Thalassaemia Unit in each district. The College of Haematologists as well as colleges of other specialities have already had discussions with the Ministry of Health Services. A plan is now being drawn up to manage Thalassaemia at a national level. Q. Will you be carrying out an awareness program to educate the public as well? A. Yes. Awareness raising and educating the public about Thalassaemia is a very important part of our campaign. This is the only way we can prevent two persons with thalassaemia minor from getting married and giving birth to Thalassaemia major children, who will suffer for life for no fault of their own. Q. Thalassaemia is still not well understood by the general public. From where can one obtain more information on the subject?. A. For more information on this subject, read Dr. Nanda Premetilleke, a senior retired haemotologist's book on Thalassaemia which is available in Sinhala and English. For more information, you can contact him at the Sri Lanka College of Haemotologists, Faculty of Medicine, Colombo. |
|
| News | Business | Features
| Editorial | Security
| Produced by Lake House |

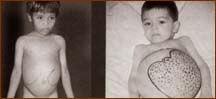 Thalassaemia is one of the most heart-breaking diseases in young
children who rarely survive till adulthood. But it can easily be
prevented, says, Prof. Arundathi Kurukulasuriya, President of the Sri
Lanka College of Haematologists in an interview with Carol Aloysius.
Thalassaemia is one of the most heart-breaking diseases in young
children who rarely survive till adulthood. But it can easily be
prevented, says, Prof. Arundathi Kurukulasuriya, President of the Sri
Lanka College of Haematologists in an interview with Carol Aloysius.




