|
  |
| Sunday, 7 November 2004 |
| Features |
| News Business Features Editorial
|
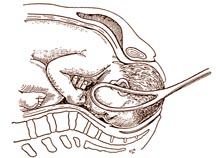
Is forceps delivery safe?
There is still a lot of mixed feelings concerning a forceps and vacuum extractor delivery. Dr. Ashmore F. Attapattu, Consultant Obstetrician and Gynaecologist discusses the subject with Carol Aloysius. Q: What is meant by a forceps delivery? A: This is a delivery performed through the normal birth canal of the mother using forceps. Today most obstetricians advocate their use merely to assist the mother when the baby's head is very low down in the birth canal. Q: When is a forceps delivery indicated? A: Modern indications for a forceps delivery are very limited. In the early years of evolution of the modern forceps, deliveries using forceps were performed for a variety of indications. The 'High Forceps' is an act of the past. It was virtually used to 'fish' a head above the pelvic brim. High maternal and foetal mortality and maternal and foetal injuries were the natural outcome. Foetal mortality is between 17 to 30 per cent. The 'Mid Cavity' forceps delivery is still being performed under certain circumstances.
It is mandatory that the foetal head is completely in the pelvic cavity and other conditions for its application are fulfilled. The 'outlet and low pelvic forceps' applications are the ones most often being used today. Q: What are the conditions that should be fulfilled before the applications of forceps? A: Forceps are applied only to a foetal head. The head should have descended completely into the pelvic cavity. The membranes should be absent. The cervix (mouth of the womb) should be fully dilated. In other words the upper part of the womb, lower part of the womb and the vagina should be one continuous passage. The vertical suture line (sagittal suture) of the fetal head should be in a north-south direction. When there is a large swelling of the fetal scalp (Caput succedaneum) one has to be very cautious when determining the level to which the bony head of the fetus has descended. Many a failed forceps have resulted due to excessive force applied. High fetal mortality and morbidity are often the result. The pelvic cavity should be roomy. An episiotomy (an incision made on the perineum) should be given after infiltration with a local anaesthetic when the head is 'crowned' (head does not recede in between contractions). Q: When is it necessary to apply forceps? A: At the second, stage of labour, i.e. when the cervix is fully dilated and baby's head is fully in the pelvic cavity (with part of the head felt abdominally) and the bearing down efforts of the mother are weak, forceps application may be necessary. Generally two hours is given at this stage of labour. Sometimes in mothers having their first baby, the perineum is quite rigid and may require assistance. Similarly in mothers who have had babies, if the perineum is severely scarred, a forceps delivery may be indicated. In certain circumstances the baby's head may be arrested in the second stage of labour due to mal-rotation. This may require intervention with a special type of forceps called Kiellands Forceps for rotation and traction. In the delivery of the 'after coming head' when the baby presents by the buttocks (Breech) forceps are applied to the head for a safe delivery. Q: When is forceps delivery necessary? A: Forceps are applied as a routine when the mother has Heart and Lung Diseases in order to prevent her straining excessively. When the mother has 'maternal distress' i.e. a prolonged labour, rise of temperature and pulse, abdominal distention, instrumental intervention is necessary. This should not be seen in modern obstetrics. Forceps delivery is also advisable when the baby is premature and in 'foetal distress' i.e. when there is a rapid or slow heart beat of the baby or certain irregularities are seen in a tracing of the heart beat (CTG). Q: What injuries could a baby sustain as a result of a misjudged forceps delivery? A: Many different injuries are possible ranging from minor bruises and lacerations to major ones. Scalp, face and soft parts are the most affected. Fracture of the nose, tearing and removal of one ear are events of the past. Injuries to the eyes and fracture dislocations of the upper spinal cord have occurred with forcible forceps deliveries. Brain haemorrhages are sometimes seen. Facial paralysis as a result of compression by a blade of the forceps could occur. Complete recovery after about two weeks is the end result. Blade marks over the face generally disappear with time. Q: What injuries could the mother sustain as a result of a forceps delivery? A: The episiotomy incision on the perineum could sometimes extend and tear the muscles supporting the rectum and anus and the upper wall of the rectum. Anal sphincter laxity and fecal incontinence are sometimes seen later. Proper attention to tears in the anus, rectum, vagina, cervix, urethra is extremely important. Intercommunication of such tears could lead to fistulae resulting in urinary and fecal incontinence (involuntary escape of urine and faeces). Q: What is the vacuum extractor? A: This is a simple device consisting of suction cups, a pump and a vacuum bottle, whereby traction is applied to the fetal scalp during the delivery of a baby. Q: Under what circumstances is the vacuum extractor used? A: The most important factor is the experience of the person using it. It is particularly used today when mothers opt to have their delivery under epidural anaesthesia, as the bearing down efforts of the mother are often impaired. When delay in the second stage of labour is due to mal-rotation of the baby's head, if the suction cup is properly applied followed by traction, maternal injuries seen with Kiellands Forceps could be avoided. Compared to forceps deliveries vacuum extractions are less traumatic to the mother. Q: What happens when the suction cup is applied and suction commenced? A: The suction draws into the cup the part of the scalp of the baby which is within it. This is called a Chignon. Traction is applied to this swelling. Q: Are injuries to the mother and baby seen when the vacuum extractor is used? A: Injuries to both the mother and baby could be prevented to a great extent by the proper choice of suction cups; to avoid its use when the baby's head is high up and the cervix is not fully dilated. Of course it is understood that the operation should be performed by an experienced person. It is obvious that the vacuum extractor cannot be used with a face presentation. Some prefer not to use the instrument on a preterm infant. Maternal and foetal injuries have been documented. Injuries to the perineum of the mother are less than with a forceps delivery. Mild skin abrasions to the infant could occur. These are not of any consequence. The Chignon which appears as a swelling of the scalp settles with time. Skull fractures and brain haemorrhages could occur. Q: What long term effects could babies suffer consequent to a forceps or vacuum extractor delivery? A: Most recent studies indicate that developmental delay after instrumental delivery is rare. Intelligent tests performed on such children have shown to be normal. Q: What advice could you give the young doctor who practises obstetrics? A: Every procedure in the practice of obstetrics, be it old or new has its place. Instrumentation requires good training, correct judgement and wide experience. |
|
| News | Business | Features
| Editorial | Security
| Produced by Lake House |