|

March 21 is World Down’s Syndrome Day:
Down ’s syndrome and physiotherapy
By Carol Aloysius
Down Syndrome (DS) is not a well understood illness. Although due to
more awareness raising on the part of health authorities, more parents
are now bringing their children in for treatment, to most parents and
caregivers, the health complications connected with this condition as
well as its cause, continue to baffle them.
How should these children be handled? How can their condition be
identified early? What kind of treatment helps them most and why?
Chartered Therapist Dr Gopi Kitnasamy believes physiotherapy is one of
the most effective ways of giving these children a new lease of life. He
explains why in this interview with the Sunday Observer, in which he
also answers other questions related to this medical condition.
 Excerpts... Excerpts...
Q. What is Down Syndrome? Is it widely prevalent globally?
A. Down's Syndrome is the most common chromosome abnormality
in humans, occurring in about 1 per 1,000 babies born each year. It is
named after John Langdon Down, the British doctor who fully described
the syndrome in 1866.
Q. Is it a genetic disorder?
A. Down Syndrome (DS) or Down's Syndrome, also known as
trisomy 21, is a genetic disorder caused by the presence of all or part
of a third copy of chromosome 21.
Q. What is it associated with?
A. It is typically associated with physical growth delays,
characteristic facial features and mild to moderate intellectual
disability.
Chromosomes determine how a baby grows in the mother's womb before
birth and how the baby's body functions after birth, and normally, a
baby is born with 46 chromosomes.
The extra copy of chromosome 21 in babies born with DS changes the
typical development of the brain and the body, causing mental and
physical challenges.
Q. What are the early signs and symptoms? Can they vary from
person to person?
A. The symptoms of DS include physical differences and
intellectual difficulties that continue into adulthood and can range
from mild to severe.
Q. When can they be detected?
A. DS may be detected during pregnancy by screening or
diagnostic tests. If not detected before birth, Down syndrome usually is
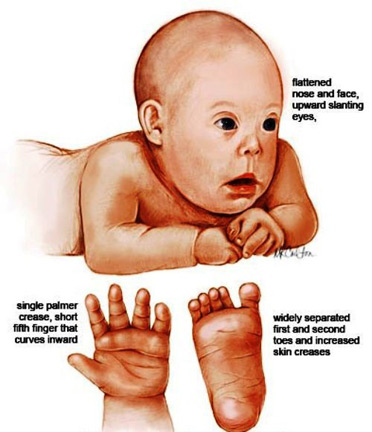
detectable at birth by the baby's physical characteristics. These
physical characteristics include:
* Low muscle tone
*A single deep crease across the palm of the hand
* A slightly flattened facial profile, and an upward slant to the
eyes.
Q. How can a doctor confirm the baby has DS?
A. A chromosomal analysis will be done to confirm the
diagnosis.
Q. How is it diagnosed?
A. Three types of DS have been identified, and all types are
diagnosed by a chromosomal analysis, frequently a blood test, ordered by
a physician.
Type 1. The most common type of DS is called “Non-disjunction Trisomy
21.” This type of DS occurs when three copies of chromosome 21 are
present in the fertilised egg. Typically, one copy of chromosome 21
comes from the father and one copy from the mother. When three copies
are present, the extra chromosome may come from either the mother or the
father. As the baby develops, the extra chromosome is copied into every
cell in the body.
Type 2. Translocation Trisomy 21 is seen in about 4 percent of all
people with DS. In this type of DS, part of chromosome 21 breaks off
during cell division of the fertilised egg and attaches to another
chromosome.
The total number of chromosomes in the cells is the usual 46, but the
extra part of chromosome 21 causes the baby to have the characteristics
of DS.
Type 3. Mosaic Trisomy 21 occurs in about 1 percent of persons with
DS. This type of DS occurs when a “nondisjunction” of chromosome 21
takes place in 1 of the cell divisions of the fertilised egg, but not
all cell divisions are affected.
Some of the baby's cells contain 46 chromosomes, which is typical,
but other cells contain the extra chromosome 21 for a total of 47.
People with Mosiac DS may have fewer characteristics of the syndrome.
Q. What are the adverse health problems arising from this
condition?
A. Almost 50 percent of babies born with DS will have some
type of congenital heart disease, which may be noted at the time of
birth or soon after. Natural development is often delayed because the
baby has low muscle tone (hypotonia), decreased strength, increased
movement at the joints (hyper-mobility), poor balance, posture
difficulties, feeding problems, and poor hand use. Children with DS also
often require increased time to learn complex movements, such as riding
a tricycle. Additional symptoms as the baby develops include:
* Poor language development and language use
* Vision and hearing problems
* Intellectual disability
Possible misalignment of bones at the base of the head and
compression of the spinal cord. In later childhood and adulthood, people
with DS may develop other symptoms, such as:
*Low motivation
* Difficulty learning complex movement tasks
* Obesity
*Poor cardiovascular health
*Thyroid dysfunction/diabetes
* Skin disorders
* Sleep apnea
* Depression
* Early onset of dementia
Q. You mention body movements are badly hampered. How does a
physical therapist help give these children more mobility?
A. Down Syndrome children want to do what all children want to
do: they want to sit, crawl, walk, explore their environment, and
interact with the people around them.
To do that, they need to develop their gross motor skills. Because of
certain physical characteristics, which include hypotonia (low muscle
tone), ligamentous laxity (looseness of the ligaments that causes
increased flexibility in the joints) and decreased strength, children
with Down syndrome don't develop motor skills in the same way that the
typically-developing child does.
They find ways to compensate for the differences in their physical
make-up, and some of the compensations can lead to long-term
complications, such as pain in the feet or the development of an
inefficient walking pattern.
The goal of physical therapy for these children is not to accelerate
the rate of their development, as is often presumed, but to facilitate
the development of optimal movement patterns. This means that over the
long term, you want to help the child develop good posture, proper foot
alignment, an efficient walking pattern, and a good physical foundation
for exercise throughout life.
Q. What do you do in a typical physiotherapy session?
A. First, I observe what skills the child has already mastered
on his or her own. Then I determine what the child is ready to learn
next. It's critical that we teach children what they're ready to learn
within the next month rather than work on something that's too advanced
for them.
Once I know what skill the child is ready to learn, I develop a way
to teach him that skill. I break the skill down into its component
parts, and then I practice the skill with a variety of strategies to
test with which method the child is most successful. The strategies are
based on the child's learning style and physical make-up.
Q. Since this is obviously specialised training, do you give
their caregivers and parents a similar training as well?
A. Training their caregivers and parents is extremely
important as these children depend on them to gain their mobility. I
teach the parents how to practice the skill with their child. The
parents can practice the skill when the child is feeling rested and
strong, and the skills can be incorporated into the daily routine.
Through practice and repetition, the child will develop strength and
efficiency, leading to mastery of the skill.
Q. Down syndrome children are said to be temperamental. How
does temperament of the child impact on the physiotherapy given?
A. Temperament is a person's characteristic manner of
thinking, behaving and reacting. I look at a child's pattern of
thinking, behaving and reacting when learning gross motor skills. It is
my observation that children with Down Syndrome fall into two basic
categories of temperament: motor-driven and observer.
Children who are motor-driven tend to be risk-takers. They like to
move fast and tolerate new movements and positions.
They do not want to stay in one place and dislike being stationary.
Children who are observers are more cautious, careful, and want to be in
control.
They prefer stationary positions and are easily frightened when
learning new movements.
When children who are motor-driven are learning how to walk, for
example, they will take risks to take independent steps and will be
undeterred by frequent falls.
Observers will be more cautious and will only risk independent steps
when they are sure of their balance. Understanding your child's
temperament and what motivates him will help you be more effective in
helping him learn gross motor skills. You will know in advance which
activities he is likely to enjoy and which activities he is likely to
resist. Knowing this, you can begin with activities he enjoys and only
move on to more difficult ones when he is well rested and motivated to
learn.
Q. What are some general tips that parents should keep in mind
when working with their child on cross motor skills?
A. The development of gross motor skills is the first learning
task that the child with Down Syndrome and his parents will face
together.
This is an opportunity for parents to begin to understand how their
child learns. Use these tips as a starting point to begin to explore
your child's learning style. Determine what motivates your child. Your
child is more likely to move when there is something motivating him. For
example, he may crawl to get to a favourite toy.
When practicing motor skills, your child's success and enjoyment will
depend on how you play, what types of toys you use, and where you place
them.
Think how your child thinks. Figure out what gross motor skills your
child likes to do and then build on those skills. For example, if your
child likes to be on his belly, teach him pivoting, crawling and
climbing; if he likes to sit, teach him to move into sitting by himself.
Children often are motivated to learn skills in a different order and
it is OK to follow your child's lead and work on what he is ready and
willing to learn.
Set your child up to succeed. Practice skills that your child is
ready to learn so that he can accomplish them.
Practice when he's at his physical best so that he has the energy,
concentration and patience to work on new or emerging skills.
Know how to position him and use the best motivators. Lastly, know
when to quit.
A few well-timed moments when your child understands a new skill and
succeeds at it are much more valuable than an hour of struggling that
leaves both of you frustrated and upset.
Read your child's cues. Pay attention to how your child is responding
to practicing the skills. If it is too hard, make it easier by changing
the set-up or giving more support.
Q. What if the child does not come upto a parents’
expectations? What more can a parent do to motivate the child to do
better?
A. Practice as long as your child is doing his best. The
quality of time you spend practicing gross motor skills is much more
important than the quantity.
Treat it as a game. You really want to think of teaching and
practicing a skill as a game.
First, introduce the “game” so your child feels and tolerates the
movement. Second, help your child become familiar with the game and
understand what you want him to do. Third, practice the game together
and gradually lessen your support. Fourthly, progress toward
independence.
The ultimate goal is for your child to master the game and be able to
do it on his own.
Q. How will you describe the way a DS child learns and the way
a normal child learns?
A. Children with Down Syndrome have a unique learning style,
and we need to understand and respect it. Well-known psychologist
Jennifer Wishart, an authority on this subject says, “we could run the
risk of changing slow but willing learners into reluctant, avoidant
learners.”
Q. Are your exercises and physiotherapy sessions tailor made
to suit each child?
A. I customise the work I do with each child.
I make sure the Physiotherapy sessions provide a pleasant learning
environment for children so that they are willing learners, and I
encourage parents to do the same at home.
Q. Your message to parents?
A. If your child feels imposed upon, he or she is just going
to find ways to resist and avoid learning.
Q. Your wish for all Down Syndrome children?
A. I can only endorse this year's theme of ‘Health and Well-being and
Access and Equality for All.’ Down Syndrome children like other children
should be able to enjoy their life to the fullest. Given the support
structures they require to maintain good health and mobility, and most
importantly, freedom from social stigma there is no reason why they
should not enjoy that right.
Researchers discover ‘Violence gene’ linked to children
The specific gene variant has also been linked to ADHD in a new study
of five to nine year olds
A ‘violence’ gene causes some children to be attracted to high
intensity video games and films, researchers have claimed.
Dutch academics linked a gene variation to young people who sought
and engaged with violent media.
1,612 parents of children aged five to nine noted how much violent TV
their children viewed, as well as how long they spent playing violent
video games, as part of the study.
DNA samples collected at the children's birth were then analysed to
identify the gene variant.
The researchers found that children carrying a specific variant of
the serotonin-transporter gene on average consumed more violent media.
Those with the gene were also more likely to display ADHD-related
behaviours. Sanne Nikkelen of the University of Amsterdam's School of
Communication Research said: “Our results indicate that children's
violent media use is partly influenced by genetic factors.
“This could mean that children with this gene variant are more likely
to seek out stimulating activities, such as violent television viewing
and video game playing.
She said: “It is important to study the relationship between media
use and ADHD-related behaviours because children who show increased
ADHD-related behaviours often face peer and academic difficulties and
are at increased risk for substance abuse.
“Examining factors that may contribute to the development of these
behaviours is essential.”
The Independent
You can die of a broken heart, say scientists
The grief of losing a loved one doubles the risk of a heart attack,
according to a study
From Shakespeare to Twilight, the devastating effects of a broken
heart pervade popular culture - and scientists have said that you really
can die from the trauma of losing a loved one.
Grief doubles the risk of suffering a heart attack, and has the same
effect on the chances of suffering a stroke, a study has found.
Scientists at St George's, University of London, looked at GP data on
thousands of individuals aged 60 and over, some of whom had recently
lost partners.
They found that 16 per 1,000 patients suffered a heart attack or
stroke within 30 days of a partner's death - double the rate for those
whose loved ones remained alive.
The heightened risk among bereaved men and women starts to fall after
30 days, according to findings published in JAMA Internal Medicine.
Lead researcher Dr Sunil Shah said: “We often use the term a ‘broken
heart’ to signify the pain of losing a loved one and our study shows
that bereavement can have a direct effect on the health of the heart.”
He said: “There is evidence, from other studies, that bereavement and
grief lead to a range of adverse responses including changes in blood
clotting, blood pressure, stress hormone levels and heart rate control.
“All these will contribute to an increased risk of events such as
heart attacks and stroke after loss of a partner.
“In addition, we have found, in another study, that in the first few
months after bereavement, individuals may not consistently take their
regular preventive medication, such as cholesterol-lowering drugs or
aspirin.
“Sudden short-term interruption of such regular medication may also
contribute to the increased risk of cardiovascular events.
“We think it is important that doctors, friends and family are aware
of this increase risk of heart attacks and strokes so they can ensure
care and support is as good as possible at a time of increased
vulnerability before and after loss of a loved one.”
- The Independent
|









")




