 |
 |
| ||
|
|
||||||||||||||||||
|
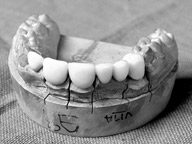
A person may lose teeth due to congenital reasons, due to the impact of a trauma or extraction. There are several methods to replace missing teeth. Dentures"Dentures are one of the cheapest methods to replace missing teeth" says Dr. Priyake Palipana "which is also not very hygienic and comfortable." BridgesBridging is a permanent prosthesis that can replace up to five teeth at a time. "Literally a bridge is something that connects two banks" says Dr. Palipana. More expensive than dentures, a bridge is a false tooth that leans on natural teeth on either side. For aesthetic reasons a certain number of natural teeth is compulsory. Lack of natural teeth to support the bridge may also compromise the functions of teeth reducing the efficiency of biting. As Dr. Palipana explained there are two types of bridges. A conventional bridge involves the grinding of natural teeth on either side. Minimal invasive bridges require less grinding of natural teeth. Moreover a damaged or discoloured tooth can be replaced with the means of a crown. The damaged tooth is ground and a cap in the shape of the tooth is cemented to the ground tooth. However bridges are considered out of date and tooth coloured fillings are recomended for slightly damaged or discoloured teeth. Implants are often recomended when replacing lost teeth as an alternative to bridging by many dental surgeons. ImplantsAn implant is a false tooth fixed to a titanium root that is inserted into the bone, therefore does not require the presence of natural teeth. Although much more expensive a procedure than dentures or bridges implants are non invasive. But every treatment has a setback. Although these sorts of devices are not affected by lightning, does not affect X rays or cause food poisoning as some may believe, Dr. Palipana said that results of MRI (Magnetic Resonance Imaging) scans may be affected by the presence of such metallic devices, rendering them unreliable. Moreover implants are not recommended for patients with diabetes or smokers. "There is a risk that an implant may get rejected in smokers and the healing process may also be affected" explained Dr. Palipana. Orthodontics appliances
Two types of appliances are used in Orthodontics for various types of conditions - explained Dr. Sriyani Basnayake - removable and fixed. Removable appliances replace only the crown and not the root. The removable types include both the growth modification as well as appliances that move teeth. But better results can be obtained by fixed appliances. Not to mention that they are more aesthetic. Fixed appliances are fixed to individual tooth therefore each individual tooth can be moved. Fixed appliances include clear braces, a method which is used on older patients and lingual braces that are placed inside. Each treatment would take 2 to 2 and half years. "However even after the treatment retainers would have to be worn throughout life if one wants to prevent the aging process" explained Dr. Basnayake. Cleft lip and palate
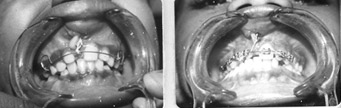
One in 600 to 700 babies is born with this condition. The cleft lip is a split in the upper lip that can range from a gap or a notch in the coloured part of the lip to a complete separation extending up the nose, from one or both sides of the upper lip. Cleft lip and palate can occur separately or together. The palate separates the mouth cavity from the nose. A split may occur in the soft portion of the palate or the hard bony palate. The split is sometimes covered by a thin membrane which is referred to as the sub mucous cleft palate. In some minor cases surgery is not required at all. For babies with clefts feeding may prove difficult because they cannot create a vacuum in order to suckle and may need additional help. These children may also have speech difficulties, since their soft pallet may not be able to perform normal function such as controlling the air escape. Such delays in speech development could have serious psychological repercussions on a child. But there is more than that meets the eye in such a condition. Children with clefts could have hearing problems as well, since there could exist a malformation in the tube that connects the throat and the ear. This could lead to what is called the 'glue ear', through the accumulation of excess fluids in the middle ear. These children are susceptible to frequent ear infections after common cold and other respiratory tract infections, and if left untreated could lead to deafness. Cleft pallet could also result in mal-alignment of teeth, which could prove difficult to clean, in which case the cleft in the bone has to be filled. Children with clefts are prone to physical as well as psychological problems and therefore require special attention. Consequently the treating children with clefts involve a multi-disciplinary approach. Surgical restoration is only part of the procedure. Cleft lip and the front of cleft palate is performed at the age of three months. The repair of the palate is done before the baby reaches one year. The palate is repaired in layers and muscles reconstructed to improve speech. Even with surgery children with clefts have a tendency to develop 'cross bite' (upper teeth fit inside lower). As the child grows older the growth of the upper jaw may be less than that of the lower jaw. In which case the cross bite would be more pronounced. Treatment which involves moving the teeth into place will be done using orthodontic appliances, usually during 8 to 9 years of age, when secondary teeth start to form. A bone grafting operation will be done - between 8 and half to 10 years of age - in case of a cleft palate that requires the restoration of the jaw and would also improve the appearance of the nose. Common paediatric neurological disorders
Dr. Phuah Huan Kee, Paediatric Neurologist of Singapore Baby and Child Clinic, Mount Elizabeth Medical Centre elaborates on 'Common Paediatric' Neurological Disorders at a recent interview. Paediatric Neurology is a is a subspeciality that manage children with neurological disorders which Covers children till age of 16 year. Neurological disorders in children may differ from those of adults so it is necessary to have paediatric neurologists who are familiar with examination of children who are aware of developmental milestones of children at various ages.In children a different spectrum of neurological disorders: * Congenital brain malformation * Neurometabolic disorders * Neurodegenerative disorders * Neurobehavioural disorders (ADHD, Autism) Common Paediatric Neurological disorders are * Developmental delay (isolated/global) * Seizure disorders/Epilepsy * Movement disorders * Headaches * Neurobehavioural disorders (ADHD, Autism) * Neuromuscular disorders. Underlying causes may be genetic or acquired: Acute Neurological Emergencies * Prolonged seizure (status epilepticus) * Meningoencephalitis * Stroke * Neuromuscular paralysis (e.g. Guillaine Barre syndrome) Are they curable? Febrile seizures. Benign Rolandic Epilepsy, Tic disorders may resolve spontaneously with age. Epilepsy can be controlled with medications Cerebral palsy, neuromuscular disorders have no cure, but rehabilitation therapies are available to optimize functional status Recent Advances in medical technology such as Better imaging modalities (MRI 3Tesla, PET scan), Prolonged video-EEG recording, Improved genetic studies, Wider selection of anti-epileptic drugs have made the treatment procedure eaier. Early identification is crucial as it leads to early intervention, Prognostication and Genetic counselling
|
|




 A smile speaks volumes, but very few people are blessed with the
perfect smile. What most don't know is that you don't have to be borne
with a perfect smile.
A smile speaks volumes, but very few people are blessed with the
perfect smile. What most don't know is that you don't have to be borne
with a perfect smile. 





 One of the major and most common problems encountered by doctors
today is the cleft lip and palate, the causes for which are still
unknown.
One of the major and most common problems encountered by doctors
today is the cleft lip and palate, the causes for which are still
unknown. 











