|

Immunisation back on the health map
By Nilma DOLE
|

Dr. Sudath Peiris
|
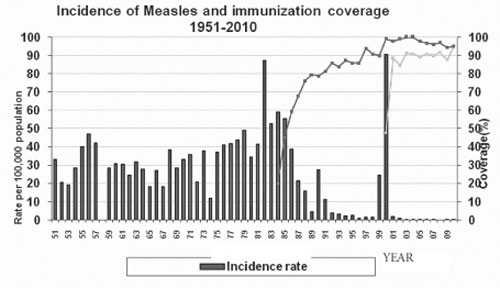
 Immunisation against vaccinable preventable diseases is a health
achievement that Sri Lanka prides itself on with no cases of smallpox
and the last reported case of polio in 1993 among other immunisation
achievements. There is always interest in immunisation because of the
benefits of injecting a little vaccination to stop some of the world’s
deadliest diseases and Sri Lanka has been one of the best countries in
the world for making full use of immunisation methods and implementing
it in a national immunisation program. Immunisation against vaccinable preventable diseases is a health
achievement that Sri Lanka prides itself on with no cases of smallpox
and the last reported case of polio in 1993 among other immunisation
achievements. There is always interest in immunisation because of the
benefits of injecting a little vaccination to stop some of the world’s
deadliest diseases and Sri Lanka has been one of the best countries in
the world for making full use of immunisation methods and implementing
it in a national immunisation program.
Be it smallpox, polio or even rubella, immunisation has saved us from
getting terribly sick and being less of a health burden for our country.
Consultant epidemiologist, Dr. Sudath Peiris of the Epidemiological
Unit, Ministry of Health explained about the the history, introduction
and new developments of the Mumps/Measles/Rubella (MMR) vaccine into the
National Immunisation Program. The problem is that Sri Lankans have
never seen the consequences of diseases so they don’t understand the
gravity of the problem. Hence, the rubella controversy sparked a fear
among the public that finally spurred some rubella cases. However, with
changes in the national immunisation policy and the public restoring
their faith in the immunisation system, Sri Lanka can be successful at
eradicating diseases which are vaccine-preventable.
 Speaking at the Health Education Bureau at an immunisation seminar,
Dr. Peiris elaborated more about the importance of immunising against
mumps, measles and rubella. He said, “The mumps virus belongs to the
family Paramyxoviridae and only one serotype of mumps virus exists.
Humans are the only known natural host for mumps virus and the virus is
spread via direct contact or by airborne droplets from the upper
respiratory tract.” He said that the incubation period averages 16 to 18
days with a range of two to four weeks where the sufferers can have
myalgia, headache, malaise and low-grade fever followed by the
characteristic unilateral or bilateral swelling of the parotid glands
(located behind the cheeks). “Unless complications occur, the illness
resolves completely because in approximately 30 percent of the cases,
infection passes with non-specific symptoms only or without symptoms at
all,” he said. Speaking at the Health Education Bureau at an immunisation seminar,
Dr. Peiris elaborated more about the importance of immunising against
mumps, measles and rubella. He said, “The mumps virus belongs to the
family Paramyxoviridae and only one serotype of mumps virus exists.
Humans are the only known natural host for mumps virus and the virus is
spread via direct contact or by airborne droplets from the upper
respiratory tract.” He said that the incubation period averages 16 to 18
days with a range of two to four weeks where the sufferers can have
myalgia, headache, malaise and low-grade fever followed by the
characteristic unilateral or bilateral swelling of the parotid glands
(located behind the cheeks). “Unless complications occur, the illness
resolves completely because in approximately 30 percent of the cases,
infection passes with non-specific symptoms only or without symptoms at
all,” he said.
There is no specific therapy or cure for a mumps infection. “Natural
infection confers lifelong protection against the virus but recurrent
mumps attacks have been reported,” he said. It hasn’t been proved
whether boosting the circulating wild virus in the community is a
prerequisite for lifelong immunity but research is on-going.
“Asymptomatic pleocytosis in the CSF (Cerebrospinal fluid pleocytosis)
is found in 50 to 60 percent of mumps patients,” he said. According to
him, symptomatic aseptic meningitis is reported in up to 15 percent of
the cases. “Mumps encephalitis (without signs of meningitis) can occur
in 0.02 to 0.3 percent of all mumps cases and deafness can occur in
about 25 percent of such cases,” he said. He said that acquired
sensorineural deafness instigated by mumps is one of the leading causes
of deafness in childhood affecting approximately five in 100, 000 mumps
patients. “Mumps orchitis occurs in 20 to 50 percent of post-pubertal
males,” said Dr. Peiris.
He said that orchitis is not associated with permanently impaired
fertility but a history of mumps orchitis may be a risk factor for
testicular cancer. Moreover, the biggest threat of mumps is in pregnancy
which would mean big problems in the long run. “If mumps is contracted
during the first 12 weeks of pregnancy, there is a 25 percent incidence
of spontaneous miscarriages,” said the doctor.
There is even a possibility of acquiring pancreatitis as a
complication in approximately four percent of the cases reported. The
disease burden of mumps burns a huge hole in the pocket of the Sri Lanka
health budget. “The estimated mumps disease burden in Sri Lanka amounts
to 20,000 to 200,000 annually in Sri Lanka. This gives rise to 280,000
cases which amount to 2.8 million days of disability,” said Dr. Peiris.
The present WHO (World Health Organisation) recommendations on the MCV1
(Measles containing vaccine) depends on epidemiology and programmatic
considerations. According to specifications, the first dose is
administered at nine months where infants were prone to disease and two
doses given when the infant is between the age of six and nine months.
The present WHO recommendations state that in order to ensure optimum
population immunity, all children should be given a second opportunity
for measles immunisation. Dr. Peiris said, “This is plausible because it
should help reduce the number of unvaccinated children and to reduce
primary vaccination failures (vaccinated children who do not
seroconvert).” This is generally administered at the age of four to six
years but the second dose may be given as early as one month following
the first dose, depending on local programmatic and epidemiological
situation.
 “The coverage of 95 percent for the first dose and 80 percent for the
second dose is listed by a panel of experts as one of five indicators of
progress towards regional elimination of measles. “The coverage of 95 percent for the first dose and 80 percent for the
second dose is listed by a panel of experts as one of five indicators of
progress towards regional elimination of measles.
The second opportunity plays important role in increasing proportion
of population with lifelong protection against measles, as boosting
through natural infection gradually disappears,” said Dr. Peiris.
The existing Mumps Vaccine WHO Recommendations states that the first
dose of the mumps vaccine should be given at the age of 12 and 18
months. The proposed MMR Vaccine schedule will commence from October 1,
2011 for the first dose at the age of one and the second dose at three
years.
“The proposed changes to the National immunisation schedule will
commence from October 1, 2011. This won’t be any different to the
traditional immunisation procedure but an update of the existing
immunisation program,” said the epidemiologist.
The measles vaccine starts from nine months to one year as the first
dose of MMRV, then the LJEV (Japanese encephalitis) vaccination is given
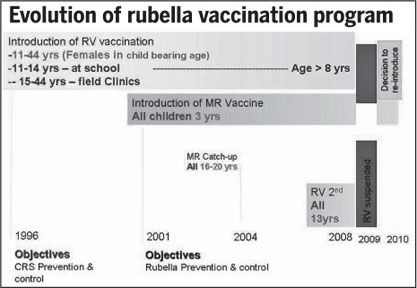
as the first dose from one year to nine months and finally, the MR
vaccine is given at three years as a second dose of the MMR. “The MMR
vaccine could be offered to females in child bearing age (16 to 44
years) as a rubella containing vaccine instead of the traditional
rubella vaccine,” said the doctor.
At present, the measles vaccine schedule offers the first vaccination
opportunity at nine months as the measles vaccine.
The second opportunity is at three years as the measles/rubella
vaccine. In the rubella, the first opportunity is administered at nine
months as the measles vaccine and the second opportunity is at three
years as the MR vaccine. With changes in the National Immunisation
program, the public shouldn’t worry if it is successful. Countries in
Europe and America have been following the updated immunisation policies
for years with success.
“If we want to make our country successful, we should start by
creating a healthy nation free of disease and those who are not a burden
to our health sector financially.
In this way, immunisation is the way forward in creating a nation
free of disease,” said Dr. Peiris.
Deadly link between high salt intake and obesity
 Dietary salt intake and obesity are two important risk factors in the
development of high blood pressure. Each packs its own punch, but when
combined, they deliver more damage to the heart and kidneys than the sum
of their individual contributions. Dietary salt intake and obesity are two important risk factors in the
development of high blood pressure. Each packs its own punch, but when
combined, they deliver more damage to the heart and kidneys than the sum
of their individual contributions.
Discovering the molecular mechanisms behind this lethal synergy has
presented a challenge to scientists, but research led by Toshiro Fujita,
MD, suggests that high dietary salt intake and obesity work together to
trigger an abnormal activation of a cellular protein called Rac1.
Obesity and a high-salt diet
Dr. Fujita’s team studied the effects of a high-salt diet in rats
bred to have high blood pressure and different levels of blood pressure
sensitivity to salt.
When obese “salt-sensitive” rats were fed a high-salt diet, the team
found that Rac1 activated the mineralocorticoid receptor (MR) on the
rats’ kidney cells. This receptor is normally activated by the hormone
aldosterone. When turned on, MR leads to the expression of a protein
called epithelial sodium channel (ENaC) and an enzyme called the sodium
pump. Both of these substances promote the reabsorption of salt, which
causes the body to retain fluid and results in high blood pressure.
wThis is the first time scientists have seen Rac1 usurp aldosterone’s
role in activating MR in the regulation of blood pressure. The protein’s
usual duties entail regulating an array of cellular events such as cell
growth. The team made the discovery when attempting to treat the obese,
hypertensive rats with drugs designed to block MR activation and inhibit
Rac1. When Rac1 inhibitors were successful in lowering the rats’ blood
pressure, the team knew they had discovered a mechanism by which obesity
and a high-salt diet team up to wreak havoc on blood pressure and the
kidneys.
Findings
According to Dr. Fujita, the team’s findings carry important
implications for the treatment of hypertension. “Our data indicate that
the Rac1-mediated pathway in the kidneys can be an alternative
therapeutic target for salt-sensitive hypertension and salt-mediated
kidney injury,” he said.
“Based upon our results, we can speculate that Rac1 in the kidneys
regulates salt susceptibility of blood pressure, and that Rac1
inhibitors, as well as MR antagonists, may be effective in the treatment
of salt-sensitive hypertension.”
- Japan Department of Internal Medicine
Genetic factors behind high blood pressure
 High blood pressure is a well-known risk factor for heart disease.
Researchers at the Sahlgrenska Academy at the University of Gothenburg,
Sweden, have participated in an international study of 200,000 Europeans
which has identified 16 new genetic variations that affect blood
pressure. The discovery, presented in Nature, is an important step
towards better diagnostics and treatment. High blood pressure is a well-known risk factor for heart disease.
Researchers at the Sahlgrenska Academy at the University of Gothenburg,
Sweden, have participated in an international study of 200,000 Europeans
which has identified 16 new genetic variations that affect blood
pressure. The discovery, presented in Nature, is an important step
towards better diagnostics and treatment.
A billion people worldwide suffer from high blood pressure and are
therefore in the danger zone for the likes of heart disease and stroke.
Effective prediction and control of high blood pressure is therefore one
of the most pressing global health issues.
Analyzing genetic data
Researchers from the Sahlgrenska Academy at the University of
Gothenburg are among an international consortium of more than 400
researchers from the US, Europe, Asia and Australia hoping to identify
which parts of our genes influence blood pressure by sifting through
vast quantities of genetic data.
2.5 million DNA variations
In their latest study, the researchers analysed more than 2.5 million
DNA variations from more than 200,000 Europeans.
The results, published in the renowned journal Nature, reveal 16
previously unknown genetic regions with interesting genes that regulate
the body’s blood pressure both the lower level when the heart expands
(diastolic) and the upper level when the heart contracts (systolic).
Genetic risk groups
With the help of these newly discovered genetic variations, the
researchers have constructed genetic risk groups to help predict the
risk of strokes and heart attacks.
“We’ve been able to classify individuals on the basis of how many
risk variants for hypertension they have in their genes” says Fredrik
Nyberg, a researcher from the Sahlgrenska Academy working on the
project.
Important step forward
In another study published at the same time in Nature Genetics, the
researchers from Gothenburg identify additional new genetic regions and
genes controlling two other measures of blood pressure: pulse pressure
(the difference between systolic and diastolic) and mean arterial
pressure (an average of systolic and diastolic).
The study shows how important it is to analyse different measures of
blood pressure. For example, pulse pressure is a marker of rigidity in
the arteries carrying blood from the heart to the body, and different
genes seem to control different aspects of blood pressure.
The results of the two studies are considered to be an important step
towards understanding how the body regulates blood pressure, and the
newly discovered genetic regions are potential targets for future
treatments.
- M.N.T.
Yawning, not just a sign of sleepiness
Though considered a mark of boredom or fatigue, yawning might also be
a trait of the hot-headed. Literally.
A study led by Andrew Gallup is the first involving humans to show
that yawning frequency varies with the season and that people are less
likely to yawn when the heat outdoors exceeds body temperature. Gallup
and his co-author Omar Eldakar report in the journal Frontiers in
Evolutionary Neuroscience that this seasonal disparity indicates that
yawning could serve as a method for regulating brain temperature.
Gallup and Eldakar documented the yawning frequency of 160 people in
the winter and summer with 80 people for each season.
They found that participants were more likely to yawn in the winter,
as opposed to the summer when ambient temperatures were equal to or
exceeding body temperature. The researchers concluded that warmer
temperatures provide no relief for overheated brains, which, according
to the thermoregulatory theory of yawning, stay cool via a heat exchange
with the air drawn in during a yawn.
Gallup describes the findings
This provides additional support for the view that the mechanisms
controlling the expression of yawning are involved in thermoregulatory
physiology. Despite numerous theories posited in the past few decades,
very little experimental research has been done to uncover the
biological function of yawning, and there is still no consensus about
its purpose among the dozen or so researchers studying the topic today.
“Enter the brain cooling, or thermoregulatory hypothesis, which
proposes that yawning is triggered by increases in brain temperature,
and that the physiological consequences of a yawn act to promote brain
cooling.
“I participated in a study that confirmed this dynamic after we
observed changes in the brain temperature of rats before and after the
animals yawned.
“The cooling effect of yawning is thought to result from enhanced
blood flow to the brain caused by stretching of the jaw, as well as
countercurrent heat exchange with the ambient air that accompanies the
deep inhalation.
“According to the brain cooling hypothesis, it is the temperature of
the ambient air that gives a yawn its utility.
“Thus yawning should be counterproductive - and therefore suppressed
- in ambient temperatures at or exceeding body temperature because
taking a deep inhalation of air would not promote cooling. In other
words, there should be a ‘thermal window’ or a relatively narrow range
of ambient temperatures in which to expect highest rates of yawning.
“To test this theory in humans, I worked with Omar Eldakar to conduct
a field-observational experiment that explored the relationship between
ambient temperature and yawning frequency. We measured the incidence of
yawning among people outdoors during the summer and winter months in
Arizona. Summer conditions provided temperatures that matched or
slightly exceeded body temperature (an average of 98.6 degrees
Fahrenheit) with relatively low humidity, while winter conditions
exhibited milder temperatures (71 degrees Fahrenheit on average) and
slightly higher humidity. We randomly selected 160 pedestrians (80 for
each season) and, because yawning is contagious, had them view images of
people yawning.
“Our study accordingly showed a higher incidence of yawning across
seasons when ambient temperatures were lower, even after statistically
controlling for other features such as humidity, time spent outside and
the amount of sleep the night before. Nearly half of the people in the
winter session yawned, as opposed to less than a quarter of summer
participants.
-US National Institute of Health
|













")
