|

Early intervention is best form of prevention :
Dengue: treatable, completely curable
By Carol Aloysius
Dengue is rising to epidemic proportions in the country, despite
efforts to control its spread by health authorities.
Consultant Resident Physician Colombo South Teaching Hospital, Dr
Asanka Ratnayake talked to the Sunday Observer on how the disease is
caused, and the Do's and Don'ts for preventing complications.
Excerpts...
Q. Dengue is now rising to epidemic proportions. What has
caused this surge especially in the Western Province?
A. Dengue is an urban and a sub-urban disease. This is because
the aedes mosquitoes which spreads the disease thrives in highly
populated areas as it feeds on human blood. Because it is a recurring
disease, dengue fever is now considered endemic to Sri Lanka. Every year
several thousand cases are recorded. It usually peaks in June and July
when the South-west monsoons are active.
 Q. Is dengue a viral disease or is it caused by a bacteria ? Q. Is dengue a viral disease or is it caused by a bacteria ?
A. Dengue infection is caused by dengue virus. It has a number
of serotypes or subtypes all of which can cause fever and all have been
seen in Sri Lanka. They are referred to as DEN 1, 2, 3 and 4.
Q. Is it infectious? How does it spread?
A. Dengue is an infectious disease. It is spread by mosquitoes
belonging to the genus Aedes. In Sri Lanka Aedes aegypti and Aedes
albopictus are the main culprits.
Of these Aedes aegypti is the principal vector. Once the female
mosquito bites an infected human (only female mosquitoes bite humans as
blood is required only for maturation of its eggs,) the virus passes on
to the gut of the mosquito.
Over a period of about 10 days the virus replicates and passes from
the intestines to the salivary glands of the mosquito. Human infection
results from the bite of the infected mosquito.
The mosquito remains infectious for its entire 1-month life, and can
transmit infection with as few as 100 viral particles.
Aedes aegypti mosquitoes most commonly bite at dusk and dawn,
indoors, in shady areas, or when the weather is cloudy. They can also
bite at any time of day.
Q. The mosquito or virus has started to mutate rapidly in
recent years. Is this one reason for its spread?
A. The four dengue virus subtypes have been known for the last
fifty years. A fifth dengue virus has been recently discovered in an
outbreak of dengue fever in Malaysia in 2007. It has not been found in
other countries and its relevance is unknown.
Q. Who are most at risk of the disease?
A. Dengue infection can develop at any age. Although 25 years
ago dengue was a disease of mostly children in Sri Lanka, it now mostly
affects teenagers and young adults.
Very young children, elderly people, obese patients and pregnant
women are at a higher risk of developing complications. Patients with
chronic diseases like diabetes and kidney disease are also at higher
risk. Mothers with young children who tend to delay seeking treatment
and avoid admission to hospital due to social reasons too are of
increased risk having complications.
Q. What are the early symptoms?
A. Dengue virus infection is mostly asymptomatic. Hence
patients will be unaware of the illness. When it is symptomatic it can
manifest as one of two diseases:
Dengue Fever (DF) or the more severe Dengue Haemorrhagic Fever (DHF).
It's difficult to distinguish between the two conditions during the
first few days of the illness.
Patients who develop dengue for the first time generally develop DF.
Patients who have had the illness previously have a high chance of
developing DHF. However most patients may not recall a previous dengue
episode as most primary infections are asymptomatic.
The reason for a second or a subsequent infection to be more severe
is because antibodies formed after infection with a particular subtype
can increase the disease severity when infected with a different dengue
virus subtype.
Symptomatic dengue presents with fever which is usually of high
grade. Headache, backache, joint pains and muscle pains are very common
and prominent and present early.
The fever can go on for three to seven days (rarely longer) and the
patients are likely to develop poor appetite, nausea and vomiting. Some
can occasionally have diarrhoea on presentation which can be mistaken
for gastroenteritis. Evidence of bleeding such as gum bleeding, skin
patches and conjunctival bleeding are seen in some during the first few
days.
Stages
Dengue fever has two stages: the Febrile (fever) stage and
Convalescent stage. Patients enter the Convalescent stage as the fever
recedes and show dramatic clinical improvement and regain the appetite.
Their laboratory parameters also improve at the same time.
In contrast, in Dengue Haemorrhagic Fever (DHF) after the febrile
stage the patients enter a period known as the critical stage. During
this stage the blood vessels become porous and fluid (serum) starts to
leak from the circulation into the pleura and the peritoneum (potential
spaces around the lungs and the bowels respectively). They can also
bleed large amounts especially into the stomach and the intestines. This
may manifest as bloody or brownish vomits or tar like stools. It is
during this stage that the patient's blood pressure can drop, breathing
can become difficult and eventually collapse if not treated. Most
patients develop some degree of liver involvement.
Q. How do you differentiate between dengue and normal viral
flu?
A. Initially it may be difficult to clinically differentiate
dengue from other viral infections. Headache, backache and muscle pains
are commoner in DF compared to “viral flu”. Upper respiratory symptoms
like sneezing and blocked nose are uncommon.
Q. Is Dengue treatable? If so, what is the treatment you
initially give a patient with a suspected case of dengue?
A. Dengue is treatable and completely curable. Treatment on
admission to hospital will depend on the patient's condition and the
stage of the disease the patient is in. Treatment of acute dengue is
supportive, using either oral or intravenous re-hydration for mild or
moderate disease, and intravenous fluids and blood transfusion for more
severe cases.
The most important aspect of the management is close monitoring of
the patient's vital parameters (i.e. blood pressure, heart rate,
respiratory rate and the urine output) along with the blood counts.
The amount and the type of fluid to be given is determined according
to the above parameters, therefore it is vital that patients are
admitted to a hospital before they become unstable.
It is well known that the blood platelet count drops in dengue
infection. Platelets are needed for clotting blood. The dropping
platelets is only one of the number of many problems that occur in
dengue and it is not the main reason for bleeding.
Changes in the count is mainly used as an indicator of disease
progression. Platelet transfusions are indicated only very rarely, if at
all.
Q. What are the health impacts of getting dengue? What organs
of the body does it affect most?
A. Dengue affects most organs in the body. It affects the
blood vessels and the liver in most patients. The brain can be involved
occasionally and involvement of the heart is rare. The kidneys are not
directly damaged by the dengue virus. Unless the patient had organ
damage due to severe and prolonged shock (due to low blood pressure),
upon full recovery there will be no long term sequel due to dengue.
Q. If the fever is mild and the case is not confirmed, do you
still insist the patient is admitted or allow him/her to go home and
return of symptoms worsen?
A. As dengue is now endemic in Sri Lanka, any fever with body
aches has the possibility of being dengue. Therefore it is important to
seek medical advice early even if the fever is mild. Nevertheless all
patients need not be admitted to hospital. The physician responsible for
the patient will advise admission if blood counts (platelets and white
blood cells) continue to drop or the patient develops any warning signs.
The important warning signs are persistent vomiting, abdominal pain,
faintish feeling, lethargy and bleeding manifestations. If the vomiting
is preventing oral fluid intake its mandatory that these patients are
admitted to hospital.
Q. Are there home remedies for such patients?
A. There are no proven home remedies for dengue. Most claims
for such remedies are anecdotal or simply baseless. What is important is
to make sure that patients get adequate (but not too much) hydration and
has a normal urine passage. For an adult patient who is not vomiting or
having diarrhoea two to three litres of fluid should be given for a
period of 24 hours.
Q. What are the symptoms that indicate the disease has
progressed to a more advanced stage like DHF and DSS?
A. DHF (the severe form) and DF are considered as different
diseases from the outset.
Therefore DF does not progress to DHF. Dengue shock (DSS) is a later
stage in DHF. DHF patients will develop the warning signs described
above. If the patients goes to DSS level they will be collapsed and
confused with breathing difficulties and/or overt bleeding.
Q. How does dengue affect children?
A. Children are at increased risk of getting dehydrated if
they are vomiting and may not be as symptomatic as adults. It is very
important that they get prompt medical attention.
Q. How can you avoid cross infection occurring within the
hospital and in the same wards?
A. Cross infection is prevented by using mosquito nets in the
wards during the febrile stage.
Q. What are the hospitals specially geared to treat dengue
patients?
A. The Infective Diseases Hospital (IDH) specially caters for
dengue fever along with other infections. A special unit has also been
established at Base Hospital, Negombo. All General and Base hospitals in
the island take care of dengue patients under the supervision of
specialist consultants.
Q. Are there new medical advances in 1) identifying 2)
treating dengue?
A. Over past few years the use of dengue antigen test to
diagnose dengue infection has dramatically increased. The NS1 antigen,
the only Non-Structural protein of the virus that can be detected in
blood is used as a rapid test. It is very useful in diagnosing dengue
infection early.
The chances of getting a positive result is higher if done on day one
of fever. However this test cannot differentiate between DF and DHF.
Q. Are they available here? If so where?
A. The NS1 antigen test is commercially available in the
private sector in Sri Lanka. It is also available in limited numbers in
some major government hospitals.
Q. How long does it take for patients to obtain results of a
full blood count?
A. The Teaching Hospital Colombo South at Kalubowila has
automated facilities which can give full blood count result within a
short period of time if urgent.
Q. Your advice to the public?
A. Dengue infection can be prevented by preventing mosquito
breeding. The Aedes mosquito breeds in clear water and even a small
amount of water is enough for it to breed.
The mosquito lays its eggs on the side wall of water containers and
these eggs can remain viable up to a year and can start to breed when in
contact with water. Therefore when emptying water containers the inside
walls of these should be brushed and cleaned.
As the mosquito bites mainly during dusk and dawn use of mosquito
nets at night does not offer significant protection. However wearing
long sleeved dresses and long trousers as well as using safe mosquito
repellents are beneficial.
The most important methods in reducing dengue infections are keeping
the environment clean and taking personal protective measures.
Finally, to prevent and reduce deaths seek medical advice early from
a qualified medical practitioner if there are warning signs and don't
hesitate to admit him/her to a government hospital immediately.
Memories of drug addicts can be erased
Substance abusers could have their memories of drug addiction wiped
in a bid to stop them using illegal narcotics, an award-winning
neuroscientist has said.
According to new research by Cambridge University’s Prof Barry
Everitt: disrupting the memory pathways of drug users could weaken
powerful “compel” cravings, reduce “drug seeking behaviour” and open a
new field of addiction therapy.
|
Mysteries of the brain: Magnetic resonance scan of a head |
Prof Everitt, who is this year’s joint winner of the prestigious
Fondation (CORR) Ipsen Neuronal Plasticity Prize, said how his research
in rodents had found that targeting “memory plasticity” in rats was able
to reduce the impact of maladaptive drug memories.
He added that this knowledge could offer a radical new method of
treatment of drug addiction in humans, where researchers have already
established that the path to addiction operates by shifting behavioural
control from one area of the brain to another. This process sees drug
use go from a voluntary act to a goal directed one, before finally
becoming an compulsive act.
It was this process that Prof Everitt's research is trying to
“prevent” by targeting “maladaptive drug-related memories” to “prevent
them from triggering drug-taking and replaces”.
In humans this could potentially be done by blocking brain chemicals.
“It's the emotional intrusiveness of drug and fear memoirs that can
be diminished, rather than an individual's episodic memory that they did
in the past take drugs or had a traumatic experience,” said. “Conscious
remembering is intact after consolidation blockade, but the emotional
arousal [that] leads to drug seeking or distressing feelings of fear
that are diminished.”
His research group discovered that when drug memories are reactivated
by retrieval in the brain, they enter a pliable and unstable state. By
putting rats in this state Prof Everitt was able to prevent memory
reconsolidation by blocking brain chemicals or inactivating key genes.
In one study, the team diminished drug seeking behaviours by
obstructing a brain chemical receptor linked to learning and memory,
thus erasing memories, while in another study it found they could weaken
drug use memories by altering a particular gene in the amygdala, a brain
area processing emotional memory.
“Of course, inactivating genes in the brain is not feasible in
humans,” the professor told FENS.
“So we’re directing our research to better identify the underlying
brain mechanisms of memory reconsolidation.”
He added: “We specifically examined how we could target these
maladaptive drug-related memories, and prevent them from triggering
drug-taking and relapse.”
- The Independent
Treatment-resistant hypertension requires proper diagnosis
High blood pressure - also known as hypertension - is widespread, but
treatment often fails. One in five people with hypertension does not
respond to therapy. This is frequently due to inadequate diagnosis, as
Franz Weber and Manfred Anlauf point out in Deutsches Ärzteblatt
International.
 If a patient's blood pressure is not controlled by treatment, this
can be due to a number of reasons. Often it is the medication the
patient is on. Some patients may be taking other medicines - in addition
to their antihypertensive therapy - which increase blood pressure as a
side effect. In these cases, the treatment of the high blood pressure
appears to be ineffective, but all that would be needed is some
adjustment to the medication regimen. Then there is diet. Licorice, for
example, does increase blood pressure; so eating too much of it may
reduce the effect of the antihypertensive therapy. Likewise,
salt-sensitive patients may increase their blood pressure by eating
salt; thus they have to keep this in mind when seasoning their dishes. If a patient's blood pressure is not controlled by treatment, this
can be due to a number of reasons. Often it is the medication the
patient is on. Some patients may be taking other medicines - in addition
to their antihypertensive therapy - which increase blood pressure as a
side effect. In these cases, the treatment of the high blood pressure
appears to be ineffective, but all that would be needed is some
adjustment to the medication regimen. Then there is diet. Licorice, for
example, does increase blood pressure; so eating too much of it may
reduce the effect of the antihypertensive therapy. Likewise,
salt-sensitive patients may increase their blood pressure by eating
salt; thus they have to keep this in mind when seasoning their dishes.
Besides drugs and food, certain symptoms may interfere with
antihypertensive therapy. Once the underlying condition has been
successfully treated, blood pressure control does often improve. An
example for this is the sleep apnea syndrome: Apart from sleep problems
and fatigue, it makes high blood pressure worse. Here, most patients
find their blood pressure improved with targeted treatment of the apnea
and quite often the antihypertensive medication can be reduced.
Thus rigorous diagnostic evaluation is key to a successful treatment
of hypertension. In their current study the authors expect that with
this approach almost half of the cases classified as treatment-resistant
hypertension could be treated.
- MNT
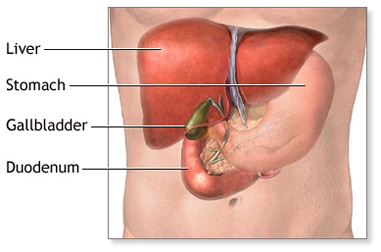
Removing gall bladder for suspected common duct stone shows benefit
 Among patients with possible common duct stones, removal of the gall
bladder, compared with endoscopic assessment of the common duct followed
by gall bladder removal, resulted in a shorter length of hospital stay
without increased illness and fewer common duct examinations, according
to a new study. Among patients with possible common duct stones, removal of the gall
bladder, compared with endoscopic assessment of the common duct followed
by gall bladder removal, resulted in a shorter length of hospital stay
without increased illness and fewer common duct examinations, according
to a new study.
Many common duct stones eventually pass into the duodenum (a section
of the small intestine just below the stomach), making preoperative
common duct investigations unnecessary. Conversely, a strategy of gall
bladder removal first can lead to the discovery of a retained common
duct stone during surgery. It is uncertain what is the best initial
strategy for treating this condition, according to background
information in the article. Pouya Iranmanesh, M.D., of Geneva University
Hospital and Faculty of Medicine, Geneva, Switzerland, and colleagues
randomly assigned 100 patients with possible common duct stones to
undergo immediate laparoscopic cholecystectomy (gall bladder removal)
with intraoperative cholangiogram (an imaging technique using a dye
injection to evaluate the common duct) or endoscopic common duct
evaluation followed by cholecystectomy, with patient follow-up of six
months.
- MNT
|









")




