A silent killer and its unknown cause
With an increasing demand for kidney transplants,
scientific uncertainty in what causes kidney diseases remains a serious
dilemma :
by Rhitu Chatterjee
A small crowd of villagers waits at a low-slung concrete school
building in Pedda Srirampuram, a village in the south Indian state of
Andhra Pradesh. The early morning air is crisp and the men and women are
dressed in light shawls and sweaters. Each holds two plastic bags-one
with their medical records, the other with a clear plastic container of
their urine. They line up to be seen by one of four young men at two
large wooden tables.
A researcher named Srinivas Rao sits at the first table. "What's your
name?" he asks a short, wiry man who is next in line. "D. Kesava Rao,"
the man replies, handing over his medical records. Rao, the researcher,
flips through the pages, noting down details. "His kidneys are not
functioning at all," Rao remarks. "Both his kidneys."
Kesava Rao, 45, has chronic kidney disease of unknown etiology (CKDu)
and depends on dialysis to survive. "Every week I undergo dialysis, four
weeks a month," Rao says. A soft-spoken man with a ready smile, Rao has
worked all his life on construction sites or coconut farms. He lived a
healthy life and hardly ever saw a doctor, he says, until a fever led to
an exam and his diagnosis. Rao didn't have diabetes or, until his
kidneys failed, hypertension, the two main causes of chronic kidney
disease worldwide. Nor do most of the other villagers who have gathered
here, all chronic kidney disease patients, waiting to get a free blood
test for creatinine, a metabolite and a proxy for kidney function, and
give samples of urine and blood for research.
Rural disease
This region in coastal Andhra Pradesh is at the heart of what local
doctors and media are calling a 'CKDu epidemic.' There is little
rigorous prevalence data, but unpublished studies by Gangadhar Taduri, a
nephrologist at the Nizam's Institute of Medical Sciences in Hyderabad,
in the neighbouring state of Telangana, suggest the disease affects 15%
to 18% of the population in this agricultural region, known for rice,
cashews, and coconuts.
Unlike the more common kind of CKD, seen mostly in the elderly in
urban areas, CKDu appears to be a rural disease, affecting farm workers,
the majority of them men between their 30s and 50s. "It is a problem of
disadvantaged populations," says Taduri, who is leading the team of
researchers in the village.
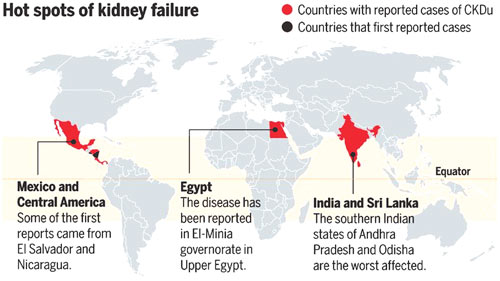
A rash of similar outbreaks in other countries has underscored that
it is a global problem. Some rice-growing regions of Sri Lanka have
their own epidemic, and the disease is rampant in sugar-producing
regions of Mexico and Central America. It has also been reported in
Egypt. Just about everywhere, prevalence numbers are scarce and
uncertain, but "there is a great deal of concern," says Virginia Weaver,
an epidemiologist at Johns Hopkins Bloomberg School of Public Health in
Baltimore, Maryland. "This is an illness that has substantial mortality.
People who would otherwise be working, raising families, are dying. It's
quite extraordinary."
Public health experts and researchers are alarmed and baffled. In
Central America, which has been hit the hardest, the leading hypothesis
is that this is an occupational disease, caused by chronic exposure to
heat and dehydration in the cane fields.
Here in Andhra Pradesh, Taduri and his colleagues think natural
toxins in the drinking water-lithium, for example-could contribute.
Using the blood and urine samples from Pedda Srirampuram, "we're going
to evaluate whether [trace elements] are really present in the body or
not," says C. Prabhakar Reddy, one of the researchers collecting the
samples.
But in India, as in Sri Lanka and Central America, researchers trying
to explain CKDu are pursuing a wide range of ideas, including excessive
use of over-the- counter painkillers and exposure to pesticides.
Nephrologist Ajay Singh of Harvard Medical School in Boston has found
high levels of silica, present in some pesticides, in the region's
drinking water, and thinks it could be responsible. "There's a smoking
gun," he says, though he concedes: "I don't know whether the smoking gun
is responsible."
As the global scale of the disease becomes clear, the search for
answers is accelerating. The beginnings of an international scientific
network to study CKDu are taking shape, and researchers are working on
simple, accurate diagnostics so that they can map incidence around the
globe-and try to correlate it with potential causes.
|

Two Indian kidney donors (Hindu) |
 |
Like most places where CKDu is rampant, India doesn't have a good
idea how many people have the disease (also known as CKDnT, for
non-traditional causes). But the anecdotal evidence from Andhra Pradesh
is sobering. We have "almost 126 widows" of men who have died from CKD,
says Rajni Kumar Dolai, the chief of the village of Balliputtuga. The
total population of his village is 3270, which implies that almost 4% of
its inhabitants have died of the disease.
By screening village populations in a van equipped with an ultrasound
machine and other diagnostic equipment, Taduri and his colleagues came
up with their estimated incidence of 15% or more in this region. Most
people diagnosed with CKDu "didn't have any complaints that suggested a
kidney problem," Taduri says. "But ... their creatinine was high."
Ultrasound exams revealed that they had "shrunken" kidneys.
Shrunken kidneys
CKDu is so deadly in part because it is hard to detect. "It is a
silent killer," says A. K. Chakravarthy, a nephrologist in Nellore,
Andhra Pradesh. In the disease's early stages, people show no symptoms.
"By the time they find out, it is too late," he says. Their kidneys are
already beyond repair, leading to high blood pressure, weakness and
other symptoms. Access to dialysis here remains limited, even though the
state government of Andhra Pradesh has added facilities in recent years.
For many patients, death comes not long after their diagnosis.
Those lucky enough to get dialysis survive for several years, but are
unable to earn a living, pushing their families deeper into poverty. His
strength and endurance sapped by the disease and dialysis, Kesava Rao
can no longer provide for his family of five. His eldest son, now 20,
has had to step into his father's shoes. "He finished high school, and
then stopped studying," Rao says. "He's the primary breadwinner of the
family now."
In India, several research groups are on the trail of a cause. But
each team has used its own methods and tools, often in isolation, making
it hard to compare findings. Taduri and Singh, for example, have both
worked in Andhra Pradesh for years, and both have pursued the hypothesis
that the high levels of silica in drinking water could be responsible.
Silica dust is known to damage lungs and kidneys when inhaled, but no
one knows what it does when ingested.
Yet the two researchers had never met until recently. "I wasn't even
aware that this work was going on," Singh says about Taduri's work.
Whereas Singh thinks the silica comes from pesticides, Taduri believes
it leaches into the groundwater from bedrock. Singh admits the
researchers could have benefitted from a collaboration. "We need to
develop a coordinated approach."
Collaborative research
 |
|
Credit for image: G.
Grullón/Science |
That is true beyond India. As scientists and public health experts
realize that CKDu is a global disease or set of diseases, they are
casting a wider net for possible causes. "We need to look at this from a
global perspective," Weaver says.
Some 30 Indian and international scientists, physicians, and public
health experts sit at a round table in a nondescript conference room at
The Energy and Resources Institute in New Delhi. The group is here for a
CKD workshop spearheaded by the La Isla Foundation, a non-profit group
that works with affected communities in Central America. The goal of the
January meeting: to create a global network of scientists studying the
disease.
The first task for the network is to determine prevalence, says Ben
Caplin, a nephrologist at University College London who works in
Nicaragua. "We need to know where are the hot spots of CKDnT," he says.
"Are there common environmental, occupational, and social factors shared
between CKDnT hot spots?"
But participants differ about how to define the disease. Caplin
proposes a working definition: "no alternative cause of CKD diagnosed by
medical professional, absence of diabetes, absence of hypertension." But
Singh says that the condition may well be a collection of diseases
caused by different factors in different places. By insisting on a
single definition, we are "already starting to have a bias on what the
causes may be."
Neil Pearce of the London School of Hygiene & Tropical Medicine, the
only epidemiologist in the room, says screening for impaired kidney
function can be done without making assumptions about causes. "We're
trying to find populations with high prevalence and low prevalence. This
says nothing about the individual."
Getting a handle on prevalence will require a standard screening
test, however. Caplin, Pearce, and their colleagues are developing a
protocol that can be adapted for different populations: a blood test for
kidney function, a urine test, and a basic questionnaire recording the
participant's age, sex, occupation and income. The team is trying to
keep it simple and inexpensive, Caplin says. "We don't want to make it
too complicated and put people off."
The team hopes to publish the protocol in a peer-reviewed journal, so
that scientists in any country can use it to screen local or regional
populations with their own funds.
"I think that using a simple protocol that will be affordable in
different settings would really shed light on the extent and global
distribution of the disease," says Catharina Wesseling, an occupational
and environmental health expert at the Karolinska Institute in
Stockholm.
Silent killer
Wesseling studies CKDnT in Central America, where it takes an even
heavier toll than in India. "Just look at the mortality numbers," says
Jason Glaser of La Isla. In Chichigalpa, Nicaragua, for example, "46% of
all male deaths are due to CKD," he says. "Seventy-five percent of
deaths of men between 35 and 55 years are due to CKD." By some
estimates, the disease has already killed at least 20,000 people in the
region.
If the disease hitting India is identical, research in Central
America could narrow the search for a cause. Recent studies there have
bolstered the hypothesis that CKDu results from long hours of work in
the heat with too little drinking water, leading to chronic dehydration.
Last year, for example, a study by Wesseling and her colleagues
showed that the disease has existed in Costa Rica at least since the
1970s, but that the death rate in Guanacaste Province has shot up from
4.4 per 100,000 men between 1970 and 1972 to 38.5 in 2008 to 2012 with
the expansion of industrial-scale sugarcane farms.
In another study, the same group showed that the kidney function of
cane cutters in one Nicaraguan community declined through a single
harvest period. "These people have a very scary deterioration of kidney
function over the harvest time," Wesseling says.
A pilot study she and her colleagues did last year hinted at how
chronic dehydration does its damage. They found high levels of uric acid
crystals in cane cutters' urine, especially at the ends of their shifts.
Those crystals could be injuring the kidneys, the researchers proposed.
"This is an important mechanism we hadn't thought about," says Richard
Johnson, a nephrologist at the University of Colorado, Denver, and an
author on the study.
But the case is far from closed. "I absolutely don't think that heat
stress and dehydration are the only part of the story," Glaser says.
"You see different severity [of the disease] in different places." Like
him, most scientists are not yet ruling out other factors.
Even before scientists know for sure what causes the disease, Taduri
says communities can take steps to reduce the risks. Providing clean
surface water sources for drinking, urging people to drink more water at
work, and advising them to stay away from pain- killers will improve
their health anyway, he contends. In El Salvador, Glaser and his
colleagues are working to expand a pilot study called the Worker Health
and Efficiency program, which prescribes frequent rest and hydration for
workers.
Fears and frustrations
Meanwhile, in CKDu-affected communities in southern India, fear and
frustration are on the rise. Now, says Taduri, villagers in Andhra
Pradesh refuse to come for screening, fearing stigma. When a man is
diagnosed with the kidney condition, "his entire family will feel him as
a burden," explains Dolai, the village chief in Balliputtuga.
On a nearby farm, a group of men stand in a circle peeling coconuts.
Most are sweating in the midmorning sun. Each stands over a blade longer
than his forearm, its wooden handle planted firmly in the soil. They
pluck coconuts from a pile and swiftly pull each one over the blade,
peeling the thick husk away from the hard, brown inner shell.
The men talk as they work, and the conversation turns to their
creatinine levels. "Mine is 1.4," says a young man in his 30s. "Mine is
1.3," another says. "One point nine."
"Two." For half the men, the levels are either borderline or high.
All work long hours under the sun, with too little water to drink.
Their legs and backs often hurt when they return home in the
evenings, and they turn to painkillers or alcohol, even though they know
both are bad for their kidneys.
The men understand they are at risk of chronic kidney disease, but
believe they can do little to stop it from progressing. Rest is not an
option, one says. "We have the disease, but we still have to work to
earn a living."
- sciencemag.org |












