 |
 |
| Sunday, 1 February 2004 |
| Features |
| News Business Features Editorial
|
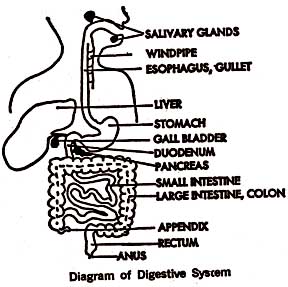
Compiled by Carol Aloysius Acute appendicitis by DR. A. M. ABOOBUCKER
Appendicitis usually occurs in both sexes and all ages are affected, but it occurs predominantly in the persons between the ages of 10 and 30 years and is more common in males. Under the age of two years it is very rare. The appendix is a small, narrow, tubular appendage in the lower-right section of the abdominal cavity. As it is a structure of worm-like shape it is more properly called vermiform appendix (worm-shaped appendix). It is usually 6 to 12 cm long and about 9 mm in diameter. It is attached to that portion of the large intestine called caecum, about two cm below the ileo-caecal valve. The caecum forms a pouch at one end and the appendix extends from this pouch closing at its far end like the finger of a glove. No useful function of the appendix is so far known. Absorption of water occurs from the lumen and accounts for the inspiration of the faecal masses which are retained in the appendix. The location of the appendix is not uniform. It shows considerable variation accounting for the variety of clinical presentation of disease. It is located behind the caecum in 65 per cent of persons, and in 30 per cent passes towards the pelvis or lies over the pelvic brim. In others it may be situated medially behind the ileum. The appendix is easily infected because of its fullness of virulent organisms, poor drainage and inadequate blood supply. Its wall contains much lymphoid tissue, the presence of which also, as in the tonsils, appears to be a factor in the localization of infection. The inflammation of the appendix is called appendicitis. Impaction of hard faeces, lodgement of a foreign body (such as orange pips, lead shot, intestinal worms or masses of undigested food), stricture or oedematous area of the appendix may cause this condition. Yet, in many instances, the primary cause of the inflammation of the appendix is not entirely understood. Appendicitis is usually acute, but it may be recurrent or chronic. Symptoms The first symptom of appendicitis is usually central abdominal pain, often accompanied by anorexia, nausea and vomiting (once or twice). The pain is sudden, intermittent, gradually progressing and of a dull aching character. The central abdominal pain is due to distention of the appendix. After several hours the abdominal pain becomes maximal and shifts to the right lower quadrant of the abdomen (right iliac fossa). In some cases the initial central abdominal pain may be of very short duration or even absent, and then the first symptom is pain in the right iliac fossa. This localized pain is due to extension of inflammation to the peritoneum over the appendix. This pain is usually associated with localized tenderness and resistance in the region of McBurney's point, one-third of the distance between the right anterior superior iliac spine and the umbilicus. The temperature may be slightly higher than normal; it rarely exceeds 100 degrees F in uncomplicated cases. The pulse rate may be normal or slightly raised. Hyperaesthesia (abnormally increased sensitivity of the skin) is sometimes elicited in the right iliac fossa due to the contact of the appendix with the peritoneum. There may also be rebound tenderness - a state in which the pain is felt on the release of pressure over the right iliac fossa. This is a very dangerous sign showing the bad condition of the appendix. Psoas and Obturator signs are also present. Gastrointestinal disturbances, constipation and absence of bowel sounds in the right iliac region are the other signs and symtoms. The appearance of a furred tongue and offensive mouth, with a typical 'alimentary' smell of breath is a very helpful sign in diagnosis the disease, particularly in children. The number of white blood cells is generally raised to 10-20 thousands per c.cm., with an increase in neutriphils. The variation in the anatomic position of the inflamed appendix may cause a different clinical picture of the disease and simulate many other diseases of the abdominal and pelvic cavities. The abdominal symptoms and signs of appendicitis are most definite when the appendix is situated in the iliac fossa or superficially located; when it lies over the pelvic brim, the abdominal pain may be minimal, with greatest tenderness on rectal examination; if it is retrocaecal the pain will be felt in the loin, with slowly developed right lower quadrant tenderness and renal disease may be simulated; if it is low in the pelvis the pain may be sited just above the pubes; if touching the ureter it may give rise to the symptoms suggestive of pyelitis; when the tip of the inflamed appendix is behind the intestine the pain may go to the back and suggest arthritis; lying under the liver may simulate inflammation of the gall-bladder. Rarely, if the appendix is long and if it is behind the maldescended caecum the pain and tenderness may be in the right hypochondrium (upper quadrant of the abdomen). In such circumstances rectal examination must be done to determine the disease accurately. Types There are two clinical types of appendicitis, catarrhal and obstructive. Catarrhal inflammation of the appendix occurs due to the damage which is done to the mucosa by a faecal concretion (faecalith) or foreign body that usually enters and goes out. Following this damage, the appendix internally becomes swollen, congested and inflamed by direct irritation given to the mucosa and externally it is reddened and turgid with flakes of organised fibrin. This type of appendicitis is characterized by the general symptoms and signs described above, and takes in many instances, a mild course. In obstructive appendicitis the lumen of the appendix is blocked by fibrosis following previous inflammation, or by a faecal concretion, foreign body, stricture, kink or oedematous area of the appendix. The obstruction is followed by inflammation, oedema and frequent infarction of the appendicular wall, which cause a rapid rise in tension in the closed portion of the appendix and result in ulceration of the mucosa and gangrene of the whole wall. All these pathological changes may occur within a few hours of the onset of symptoms. In this type of appendicitis which is more usual, the central abdominal pain is much more severe and colicky in nature. Nausea, vomiting, hyperaesthesia at early stage, and normal or subnormal temperature with normal pulse rate are the prominent symptoms of this type of appendicitis. Complications Among the complications of acute appendicitis, especially of obstructive type, the following are very important and dangerous: * Perforation * Peritonitis * Abscess formation Perforation of the appendix usually occurs due to tension in the organ or thrombosis of its arterial supply caused by inflammation. Following the perforation or rupture of the inflamed appendix peritonitis occurs when the infection spread to the peritoneum. The symptoms of these complications include severe pain, tenderness and rigidity of the whole abdomen, and a high temperature. If untreated this condition is usually fatal. Abscess formation is a common complication of untreated acute appendicitis. It usually takes place after 5-6 days of the onset. Malaise, toxicity, high fever and leucocytosis are the symptoms of this condition. Other complications include subphrenic abscess, pylephlebitis, portal pyaemia and mechanical intestinal obstruction. Treatment - the Homeopathic way Removal of the inflamed appendix (appendicectomy) is generally regarded as the only proper treatment of acute appendicitis. However, in the early stage or before complications arise with their maximal force, 70-75 per cent of the cases can successfully be cured with the homoeopathic remedies without the need of lancet. One of the following remedies may be given very frequently in suitable potency according to the symptoms until the acute symptoms subside: Bell., Bry., Dios., Iris ten., Lach., Lyc., Nat.sul., Plumb., Rhus tox, and Verat. vir. Among these Bell., Bry., and Iris ten. are most often indicated remedied. Verat. vir. Q may be applied externally. Psorinum may be given in infrequent doses, after an acute attack has subsided, to prevent the recurrence. The patient should be referred to the surgeon if marked improvement is
not evident within 6-8 hours of medical treatment. Alcohol Related Problems by Dr. D. P. Atukorale
Consumption of alcohol depends on: (a) Sex: Men are twice as likely to have alcohol related problems compared to females. (b) Occupation; Alcohol misuse is more common in jobs related to catering, brewing and distilling. (c) Homelessness: About a third of homeless people have alcohol problems. Managing Alcohol Problems Alcohol problems can present as (a) social problems (b) medical problems and (c) psychiatric problems. Most common way alcohol problems present is as social problems and include: (a) Request for medical certificates; (b) Marital problems, divorce and domestic violence; (c) Financial problems, absenteeism accidents at work' (d) Public drunkenness or aggressiveness; (e) Prosecution for violence - behaviour or driving offences and sexual assault and vagrancy. Medical problems About 80 per cent of patients referred for treatment of alcoholic misuse have important medical problems. withdrawal symptoms are often experienced on waking. Features of specific complications are extremely varied. Gastro-intestinal problems due to alcohol misuse are hepatitis cirrhosis, gastritis, gastrointestinal haemorrhage and pancreatis. All the features of depression can be induced by alcohol. Depression by itself can cause alcoholism by triggering drinking in an attempt to relieve some of the depression symptoms. Anxiety; These symptoms are often present during partial withdrawal. Just as repression, an anxiety or panic disorder can predispose to alcoholism in an attempt to relieve symptoms. Personality changes decline in the usual standards of social concern and personal care. Sexual dysfunction is quite common in alcoholics and these include impotence and delayed ejaculation. Hallucinations both auditory and visual can occur usually during withdrawal but can occur without other features of delerium tremens (D.T.). Alcoholic hallucinosis in rare. Sometimes distressing auditing hallucinations occur in people with clear consciousness. Managing Alcohol dependence Detoxification Alcohol dependence (addiction) usually requires controlled detoxification with an attenuation therapy (such as benzodiazefine). Since abrupt cessation of alcohol which occurs when an alcoholic is admitted to hospital for some other medical or surgical condition such as pneumonia or alcoholic cirrhosis and one of the withdrawal states such as DT can occur. Detoxification is increasingly taking place in the community, but, in patient detoxification is recommended for those at risk of suicide, lacking social support or giving history of severe withdrawal reactions including fits and D.T. D T is a serious condition because of associated complications such as fits, hyperthermia, dehydration, electrolyte imbalance, shock and chest infection and in hospital practice the mortality is about 10 per cent. Principles of Community Detoxification These include daily supervision in order to allow early detection of complication such as D.T., continuous vomiting or deterioration in mental state. Multivitamin preparations should be given to prevent onset of Wernickes encephalopathy. About 200mg of thiamine (vitamin B1) should be given daily by mouth to all those patients undergoing withdrawal. Serious patients will need parenteral vitamins for 3-6 days before changing over to oral therapy. Benzodiazepines should be given to prevent withdrawal symptoms. Most commonly used benzodeazefine is chlordiazepoxide at a starting dose of 10mg 4 times a day and reducing over seven days. In severe withdrawal, 40mg 4 times a day can be given at the start of treatment. Support after Withdrawal The relapse rate among alcoholics is high, but can be reduced by a programme of rehabilitation. Various options available are: (a) primary health care team. (b) Community alcohol team, (c) Residential rehabilitation programmes. (d) Voluntary organizations providing support and counselling either individually or in groups. Abstinence Disulfiram is a drug which plays a useful role to play in maintaining abstinence. Patients who take this drug experience extremely unpleasant symptoms of acetaldehyde accumulation if they drink an alcohol. Alcoholic Anonymous can provide much needed advice and support for patients and their families. |
|
News | Business | Features
| Editorial | Security Produced by Lake House |

 Appendicitis is a potentially dangerous condition and accounts for more
than half of all abdominal emergencies.
Appendicitis is a potentially dangerous condition and accounts for more
than half of all abdominal emergencies.
 In UK, alcohol consumption is associated with 80 per cent of suicides,
30 per cent of murders, 80 per cent of deaths from fire, 40 per cent of
road traffic accidents and 15 per cent of drowning. Alcohol contributes to
(a) one in 3 divorces (b) one in 3 cases of child abuse and (c) 20-30 per
cent of hospital admissions.
In UK, alcohol consumption is associated with 80 per cent of suicides,
30 per cent of murders, 80 per cent of deaths from fire, 40 per cent of
road traffic accidents and 15 per cent of drowning. Alcohol contributes to
(a) one in 3 divorces (b) one in 3 cases of child abuse and (c) 20-30 per
cent of hospital admissions.




