|

Conjoined twins- a challenge to medicine
By Husna Inayathullah
“Words cannot express the joy of new life.” - Hermann Hesse
A birth of a new born baby is a precious and memorable moment for any
family. A birth can change a family.
At times it could be a complicated and challenging experience.
The recent birth of conjoined twin girls to parents at the Mahamodara
hospital, Galle is a very rare occurrence that took us by surprise.
The parents, who already have three normal healthy children, do not
like to reveal much information about their newly born conjoined twins.
Classified under the type Omphalopagus conjoined twins, the two bodies
of the twins are fused at the lower abdomen and have two heads, four
hands and four legs according to hospital sources.
Hospital Director at Galle Mahamodara Maternity Teaching Hospital,
Dr. Priyani Senadheera says this is a rare birth of conjoined twins.
 A Caesarean surgery was conducted by Consultant Gynaecologist and
Obstetrician Priyanakari Amaradivakara on March 11, 2015. As soon as the
Caesarean was done they were moved to the hospital's Intensive Care
Unit, and later transferred to the Karapitiya hospital for further
treatment. A Caesarean surgery was conducted by Consultant Gynaecologist and
Obstetrician Priyanakari Amaradivakara on March 11, 2015. As soon as the
Caesarean was done they were moved to the hospital's Intensive Care
Unit, and later transferred to the Karapitiya hospital for further
treatment.
This kind of conjoined twin birth is a rare phenomenon estimated to
happen once in 49,000 births.
Conjoined twins are identical, but are joined in utero. It is a very
rare event with higher incidence noted in Southwest Asia, Africa and
Brazil.
Sri Lanka has experienced the birth of conjoined twins on three or
four occasions in the past 10 years, according to doctors, but
unfortunately the outcome has not been favourable.
The condition of conjoined twins is frequently found among females.
Approximately half are stillborn and a smaller fraction of pairs born
alive have abnormalities.
The origin of conjoined twins has two contradicting theories. One is
fission and the other, fusion. The fertilised egg splits partially in
fission. A fertilised egg completely separates in fusion but stem cells
find like-stem cells on the other twin and fuse the twins together.
Conjoined twins share a single common chorion, placenta and amniotic
sac.
These characteristics are not exclusive to conjoined twins as there
are some monozygotic but non-conjoined twins that also share these
structures in utero.
The most famous pair of conjoined twins in the world was Chang and
Eng Bunker in 1811 in Siam, present Thailand. They were Thai-American
conjoined twin brothers whose condition and birthplace became the basis
for the term Siamese twins. Chang and Eng were joined by a band of
flesh, cartilage, and their fused livers at the torso. They could have
been easily separated in modern times. Due to the brothers’ fame and the
rarity of the condition, the term “Siamese twins” came to be used as a
synonym for conjoined twins.
The fused liver of the Bunker brothers was preserved and is currently
on display at the Mutter Museum in Philadelphia, Pennsylvania.
Numerous artifacts of the twins including some of their personal
artifacts and their travel ledger are displayed in the North Carolina
Collection Gallery in Wilson Library at the University of North Carolina
at Chapel Hill. This includes the original watercolor portrait of Chang
and Eng from 1836.
Conjoined twins are typically classified by the point at which their
bodies are joined.
The most common types of conjoined twins are Thoraco-omphalopagus,
Thoracopagus, Omphalopagus, Parasitic twins, Craniopagus, Cephalopagus,
Syncephalus, Cephalothoracopagus, Xiphopagus, Ischiopagus,
Omphalo-Ischiopagus, Parapagus, Craniopagus parasiticus, Pygopagus and
Rachipagus.
Today most number of conjoined twins are Thoraco-omphalopagus where
two bodies are fused from the upper chest to the lower chest. These
twins usually share a heart and may also share the liver or part of the
digestive system.
A surgery is done to separate conjoined twins. Most cases of
separation are risky and life threatening. It ranges from very easy to
very hard depending on the point of attachment and the internal parts
that are shared.
Mostly the surgery results in the death of one or both of the twins
particularly if they are joined at the head or share a vital organ.
In 1957, Bertram Katz and his surgical team made international
medical history performing the world's first successful separation of
conjoined twins sharing a vital organ. Omphalopagus twins John Nelson
and James Edward Freeman (Johnny and Jimmy) were born to Mr. and Mrs.
William Freeman of Youngstown, Ohio, on April 27, 1956.
The boys shared a liver but had separate hearts and were successfully
separated at North Side Hospital in Youngstown, Ohio by Bertram Katz.
The operation was funded by the Ohio Crippled Children's Service
Society. Ben Carson made medical history by being the first surgeon to
successfully separate conjoined twins in 1987.
They were conjoined at the back of the head (craniopagus twins).
Operations to separate twins joined in this way had always failed,
resulting in the death of one or both of the infants. Carson agreed to
undertake the operation. The 50-member surgical team led by Carson
worked for 22 hours. At the end the twins were successfully separated.
Recent successful separations of conjoined twins include that of the
separation of Ganga and Jamuna Shreshta in 2001 who were born in Nepal
in 2000.
The 197-hour surgery on the pair of Craniopagus twins was a landmark
one which took place in Singapore.
The team was led by neurosurgeons, Chumpon Chan and Keith Goh.
The surgery left Ganga with brain damage and Jamuna unable to walk.
Seven years later, Ganga Shrestha died at the Model Hospital in Katmandu
in July 2009 at the age of eight, three days after being admitted for
treatment of a severe chest infection.
In 2003, two 36-year-old women from Iran, Ladan and Laleh Bijani who
were joined at the head but had separate brains (craniopagus) were
surgically separated in Singapore despite surgeons’ warnings that the
operation could be fatal to one or both.
Their complex case was accepted only because high tech graphical
imagery and modelling would allow the medical team to plan the risky
surgery.
Unfortunately an undetected major vein hidden from the scans was
discovered during the operation.
The separation was completed but both women died while still in
surgery on July 8, 2003.
Chronic cough? Weight loss? Get your chest examined :
TB is preventable and curable - Dr Bandu Gunasena
By Carol Aloysius
It was once a dreaded infectious disease which killed thousands of
men, women and children especially those living in cold climates, in the
19th century. The death toll of the White Plague was even higher than
that of the Black Plague that raged across countries killing hundreds in
its wake. The main difference is that while the White Plague is
transmitted from human to human, the former was mostly caused by rodents
(mostly rats).
With the drastic reduction of TB worldwide and in Sri Lanka which is
now ahead of most Asian countries in the WHO Elimination of TB campaign,
the Sunday Observer spoke to Consultant Respiratory Physician, National
Hospital for Respiratory Diseases at Welisara, Dr Bandu Gunesena.
Excerpts...
Q. TB was a disease that killed several hundreds of people
young and old in the 19th century to the extent it earned the name
‘White Plague'. What is TB?
|
Global statistics
|

Dr Bandu Gunasena |
TB is second only to HIV/AIDs as the greatest killer worldwide due to
a single infectious agent.
In 2013, nine million fell ill with TB and 1.5 million died from it.
Over 95 per cent of TB deaths occur in low-middle income countries and
are among the top five causes of death for women aged 15-44.
In 2013, around 550,000 children became ill with TB and 80,000 HIV
negative children died of TB.
TB is a leading killer of HIV positive people causing ¼ of all HIB
related deaths. Globally in 2013, an estimated 480,000 people developed
multi-resistant TB (MDR TB), The TB death rate dropped 45 per cent
between 1990-2013. An estimated 37 million lives were saved through TB
diagnosis and treatment between 2000-2013. |
Plague has wiped out one-third of the population of Europe during the
black plague epidemic.
A. TB is given the name white plague because the number of
deaths it has caused over centuries is much more than that of black
plague.
Q. How is it caused? By bacteria? Virus? Mosquitoes?
A. It is an air born bacterium called mycobacterium
tuberculosis which was discovered by Dr Robert Koch about 100 years ago.
Q. Is it infectious? How does it spread?
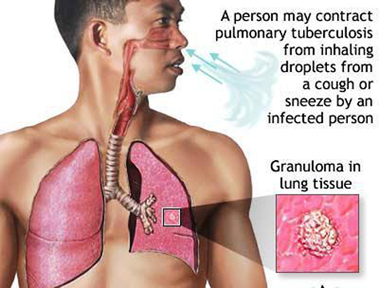
A. When an infected patient coughs out bacteria in to the
atmosphere they remain in a suspension of droplets over a long period.
When that air is breathed in by a healthy individual the infection can
begin.
Q. Are there different types of TB?
A. Yes. The TB infection can be divided in to pulmonary TB and
extra pulmonary TB.
Pulmonary TB the TB that occur in the lung and extra pulmonary means
TB of any other organ namely Brian kidney intestines.
Q. Which is the 1) most severe type? 2) The mildest form?
A. The most severe form is the TB in the brain and we call it
TB meningitis. And also TB, spreads all over the body is called miliary
TB. Since those two conditions are rare most of TB deaths occur due to
pulmonary TB. The mildest form is called latent TB and sometimes it is a
self limiting condition which heals without treatment because of very
low concentration of bacilli in the body.
Q. Are they all infectious?
A. The infectious form is the pulmonary TB which occur in the
lung, other forms do not generally transmit to others.
Q. Today, there seems to be a drastic reduction in the number
of patients worldwide and in Sri Lanka. How was this possible?
A. In fact you are wrong in that. Though there is some
reduction in TB worldwide it cannot be called a drastic reduction. In
Sri Lanka the annual incidence remained static over the past few years
and now it is showing an upward trend.
Q. In spite of the reduction, I understand new TB cases are
still emerging in Sri Lanka and elsewhere. Why?
A. The reason is sometimes due to inadequate disease
surveillance activities. But also it is due to young work force
migrating rapidly to cities and living in congested places without good
sanitary standards. Epidemics of diabetes and HIV may also contribute to
this as those two conditions make people more vulnerable to TB.
Q. As Consultant physician at the biggest hospital for
Respiratory and chest diseases in Welisara, how many new patients do you
diagnose every month?
A. My unit may be detecting about 10 patients a month and we
have three such units at Welisara
Q. How many patients do you see on a daily basis at your OPD?
A. 34 new patients have been diagnosed during the past two
months (January and February 2015) at the OPD, Welisara and 118 new
patients have been diagnosed during this period inwards at the Welisara
hospital (most of these are transferred cases from other hospitals).
Q. Are these numbers less than they were a decade ago?
A. No, we see more patients now and they present at a much
younger age than before.
Q. What are the health complications due to TB?
A. TB can technically affect any organ in the body causing
damage which can be permanent. Most commonly it causes problems in the
lung resulting in permanent scars in the lung which can lead to chronic
cough, recurrent infections, coughing out blood and finally permanent
loss of respiratory function of the lung, what is called respiratory
failure.
Q. What organs are most affected?
A. Firstly, the lung, then lymph glands, bones, joints etc.
Q. Who are those most at risk of the disease? Elderly?
Children? Those with other diseases?
A. People in both extremes of age are vulnerable. The other
condition which increase the TB risk are diabetes, alcoholism, chronic
diseases of kidneys and liver, HIV and patients after organ transplant.
 Q. According to the WHO's 2012 report an estimated 8.6 million
people developed TB and 1.3 million died of TB and related deaths. What
are these ‘related’ deaths? Q. According to the WHO's 2012 report an estimated 8.6 million
people developed TB and 1.3 million died of TB and related deaths. What
are these ‘related’ deaths?
A. The lung complications that I mentioned earlier are also
due to rare toxic effects of anti TB drugs. But any patient who dies
while being on TB treatment, is considered a TB related death even if it
is not directly related to a complication of TB.
Q. Is HIV/AIDS a TB related illness?
A. Yes. HIV makes the patient highly vulnerable to TB because
of the lowered immunity caused by HIV virus. At the same time the TB
infection will promote viral multiplication in the body and the two
conditions act synergistically to invade human body.
Q. The report also says there have been more deaths from TB
than from any other infectious disease except HIV/AIDS. Do you agree?
A. Yes, but in Sri Lanka we have more TB deaths than HIV.
Q. What are the symptoms of TB?
A. Cough, loss of appetite, low grade fever, sweating and
wasting, sometimes the patient can cough out blood.
Q. How are they detected?
A. Three early morning sputum samples are tested (examined
under the microscope) on three consecutive days for TB bacteria. Blood
tests are not used commonly in Sri Lanka. TB can be grown in a special
culture medium. It takes a minimum of six weeks to get a positive result
as the organism is a slow growing bacillus. Now there are new techniques
for rapid diagnosis but they are expensive and are not available freely.
Q. Can TB be prevented or cured if the symptoms are detected
early?
A. Early diagnosis of pulmonary TB cases can be started on
treatment promptly and the spread of the disease can be prevented. So
far there is no effective vaccination against pulmonary TB
Q. What is the standard treatment? Drugs? Surgery?
A. Sri Lanka has the drug regimen used in the developed
countries. Treatment of TB extends over a period of six months. In the
initial two months the patient is given a pill containing four drugs
combined in one pill. Patient may swallow two to three such pills a day
depending on the body weight of the patient.
In the second phase of the treatment the combination pill containing
two drugs is given for a period of four months. In patients with drug
resistant TB or those who are suspected of having drug resistance are
given longer courses of treatment.
Q. How long is the duration of the treatment?
A. For new cases the duration is six months. For patients who
relapse, an eight month of treatment is given. For multi drug resistant
TB the treatment duration is close to two years.
Q. Once a person gets TB, does he have life-long immunity? Or
can it recur?
A. Yes rarely it can recur but usually that happens if the
patient doesn't take the medicine properly as instructed or if the
patient has some immune deficiency such as diabetes HIV etc.
Q. Is smoking a cause for recurring TB? I read that a new
study published last December has said that habitual smokers (those
smoking 10 or more cigarettes or half a pack a day) have double the
chance of developing recurring TB than those who have given it up or
never smoked. Do you agree?
A. There were several small studies supporting the harmful
effects of cigarette on TB.
Q. Sri Lanka has a National Program for TB Control. What are
its goals? How does it operate?
A. The head office of national TB program is at Narahenpita.
The technical team at that office would coordinate the TB control
activities islandwide. The care is delivered to the patients by district
TB/chest clinics.
The district chest clinic will provide diagnostic services and drugs
to patients of the district and coordinate other control activities.
Q. One of the goals is to eliminate TB and increase the life
expectancy and improve the quality of life of TB patients. How does it
plan to do this?
A. By early detection of TB patients and treating them
properly and tracing the contacts and examining them to find out the
patients with early active disease.
Q. What in your opinion are the main obstacles to eliminating
TB in this country? Refusing to take medication regularly by patients?
Myths and stigma attached to TB, preventing patients from receiving or
going for treatment? Lack of screening facilities?
A. Poverty, congested living conditions, lack of awareness
about the disease.
Q. Where can an underprivileged person go to get screened for
TB free?
A. District TB /chest clinic.
Q. Your message to the public?
A. With regard to TB no one is safe until everybody is safe,
so the public has to be vigilant about people with chronic cough,
specially if they are losing weight, and if they are found, support and
help them to seek help at district chest clinics.
|













")
