Health wise
Do all heart attack patients need angiograms?
By D. P. Atukorale
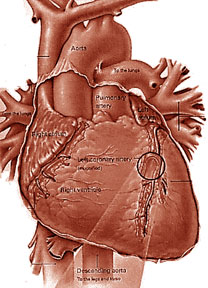
Coronary angiogram is an invasive test done for coronary heart
disease (angina and heart attack) patients and is not without risks even
in the most experienced hands and in my opinion all heart attack
(myocardial infarction) patients do not need coronary angiography test.
Majority of cardiologists go ahead with the above test only if the
Exercise E. C. G. is strongly positive (i.e grossly abnormal). A
catheter tube is passed inside the coronary arteries under local
anaesthesia by a cardiologist and a radio-opaque dye is injected in
order to visualize the coronary arteries. If the angiogram shows
evidence of major (atheromatous) blocks and if the patient has angina
which does not subside with the routine medical management, the
cardiologist usually will advise the patient to undergo
balloon-angioplasty (P.T.C.A.) or coronary artery bypass graft surgery (C.A.B.G)
if the patient can afford the expenses as all these invasive procedures
are very expensive in the private sector. Coronary angiography costs
about Rs. 35,000 and P. T. C. A. costs anything between Rs. 400,000 and
one million rupees whereas to undergo C.A.B.G. Operation, it costs about
Rs. 500,000.
 Majority of cardiologists advise their heart patients to undergo
P.T.C.A. (balloon angioplasty) if the major coronary artery blocks
involve less than three arteries and if there are more than two arteries
involved cardiologists usually advise these patients to undergo bypass
surgery which is performed under general anaesthesia. P.T.C.A. is
performed under local anaesthesia. Majority of cardiologists advise their heart patients to undergo
P.T.C.A. (balloon angioplasty) if the major coronary artery blocks
involve less than three arteries and if there are more than two arteries
involved cardiologists usually advise these patients to undergo bypass
surgery which is performed under general anaesthesia. P.T.C.A. is
performed under local anaesthesia.
All above procedures (Coronary angios, P.T.C.A. and bypass surgery)
are performed in National Hospital Colombo and some other teaching
hospitals. It should be noted that there is a waiting list for coronary
angios, P.T.C.A. and by pass surgery in the Government hospitals, and
stents (which are quite expensive) used during P.T.C.A., are very often
out of stock and the patients very often have to buy their own stents.
As mentioned earlier, if the heart patients are unwilling to undergo
P.T.C.A. or C.A.B.G, coronary angios are not usually performed. C.A.B.G.
usually has to be done within six months of doing the coronary
angiogram. If the patient is not willing to undergo P.T.C.A. or C.A.B.G,
your cardiologist will go ahead with medical treatment plus chelation
therapy (which is performed only in a few centres in Sri Lanka).
If angiography is urgently required and if you cannot afford this
test in the private sector your cardiologist will contact a cardiologist
in the government sector and will help you to get the angio done in one
of the Government hospitals.
Exercise E.C.G.
It is noteworthy that Exercise E.C.G. is sometimes not useful to
assess a coronary patient as to whether the patient needs coronary angio
because (a) Coronary angio can be normal in some patients with grossly
abnormal Exercise ECG’s and (b) A negative Exercise ECG does not exclude
serious coronary artery blocks.
A test called a “Stress-Echo” is a more useful test than the routine
Exercise ECG test and when there is a doubt in the Exercise ECG, some
cardiologists go ahead with a Stress-Echo. There are some cardiologists
who go ahead with the coronary angio even without subjecting the patient
to Exercise ECG.
Coronary angiography patients are usually admitted to hospital for 24
hours and PTCA (balloon angioplasty) patients are discharged from
hospital usually after 48 hours, and CABG patients are usually
discharged after one week or ten days.
Some patients who refuse PTCA or CABG inspite of having major
coronary artery blocks show significant clinical improvement (confirmed
by repeated Exercise ECGs) when these people undergo lifestyle
modifications and give up smoking, control their weight, diabetes, their
high cholesterol level and high blood pressure.
 In my opinion coronary angiography is highly unnecessary for majority
of heart attack patients especially of the stress testing (Exercise ECG)
is normal. In my opinion coronary angiography is highly unnecessary for majority
of heart attack patients especially of the stress testing (Exercise ECG)
is normal.
Conclusion
(a) There is no indication for coronary angiography in all heart
attack patients.
(b) Exercise ECG is a useful non-invasive test done for heart attack
patients prior to angiography.
(c) There are false positive and false negative Exercise ECG i.e.
angio can be normal in some patients with abnormal Exercise ECGs and
angio can be grossly abnormal in some patients with normal exercise
tests.
(d) Stress-Echo is a more useful test than ordinary Exercise ECG.
(e) In Sri Lanka the best test to assess patients as to whether they
need PTCA or CABG is coronary angiography, which is an invasive test and
costs about Rs. 35,000 in the private sector and in experienced hands
time taken for an angio is about 30 minutes and complications are
extremely rare.
Is now a good time to get swine flu?
No worse than a bad cold, say many of the Britons diagnosed with
swine fever. So is it time for pig flu parties, to spread a mild version
to build immunity?Dotted up and down the UK, Tamiflu has been dispensed
to swine flu sufferers and those who may have been exposed to the highly
contagious virus.
 Some fret about taking the powerful antiviral drug - with its
unpleasant side effects - and wonder if it might be wiser to catch swine
flu now, priming our bodies to fight back if a more vicious form
surfaces in winter. Some fret about taking the powerful antiviral drug - with its
unpleasant side effects - and wonder if it might be wiser to catch swine
flu now, priming our bodies to fight back if a more vicious form
surfaces in winter.
"It would be quite a dangerous thing to do," says John Oxford,
professor of virology at St Barts and the Royal London Hospitals, Queen
Mary College.
"The scenario is that you get your mates together to spread swine
flu. But then you take it home. Perhaps you take your dear old granny a
cup of tea.
She catches it. And dies." For this new version of H1N1 is highly
contagious. Someone in rude health might recover quickly, albeit after
enduring a fever, vomiting and diarrhoea. But they might pass it on to
someone less able to fight it off - someone with diabetes, asthma or a
weak immune system.
"A swine flu party would only work if you all then put yourselves in
quarantine, or returned to your hermit hole, and did not touch anyone
for at least 10 days."
Spreading germs
And while chickenpox or rubella parties were once popular as these
illnesses are more straight-forward in childhood, swine flu is in a
different league, warns Professor Oxford.
Although chickenpox can be fatal - that is rare. Dangerous
complications can happen in a small number of healthy children or those
with other chronic health problems.
People have died from swine flu and less is known about the current
strain. Health authorities don't yet know enough about it to predict how
it will affect individuals, how it will mutate and whether it will come
back.
The effects have so far been less dramatic than initially feared -
Mexico has scaled back its death toll from 159 to 56, and precautions
such as school closures seem to have slowed its spread.
But it has "full pandemic potential", the World Health Organization
says. A pandemic occurs when a new flu virus appears against which we
have no immunity, resulting in outbreaks worldwide. Already cases have
been confirmed in 30 countries, from Mexico to New Zealand, Canada to
Thailand, Germany to the UK.
"What's reassuring is that the UK has stockpiles of antiviral drugs,
enough to treat those who contract swine flu or who are exposed to it,
and to protect frontline medical staff," says Professor Oxford.
"My daughter's a GP. If [swine flu] takes off and people come in to
see her, she can take it prophylatically, one tablet a day for six
weeks."
And although swine flu is a new virus, our bodies encounter other
strains of H1N1 in the seasonal flu that does the rounds each year.
"We're not as vulnerable as we were in 1957's pandemic, which was a
totally new virus. We've come into contact with distant relatives of
swine flu before. If you catch it, your body will say 'I know this
family, I've fought off its cousin, six times removed' and go to work to
fight it off."
Prior exposure, through seasonal flu or swine flu vaccination when
one becomes available, prompts the immune system to produce suitable
antibodies to fight off the invader.
"And once exposed, you have lifetime memory of those antibodies and
can produce them again," says Professor Oxford.
Source: BBC News Magazine
Can goat’s milk cure asthma and eczema?
I refer to an article entitled “A little learning is a dangerous
thing” by Bertram Perera (BP) appearing in a popular newspaper recently.
In the above article, BP says “Asthmatics and those suffering from
chronic cough, colds and even urticaria and eczema get permanent relief
from milk of the goat”.
 I contacted two very highly qualified and highly experienced chest
physicians who have treated thousands of patients suffering from chronic
cough and asthma (bronchial asthma) in Colombo for more than 35 years.
They told me that “you can never cure or bring permanent relief to
patients with chronic cough and asthma by using goat’s milk” and that
“no physician ever treats asthma using goats milk”. The Sri lankan
Government spends millions of rupees annually importing drugs to control
bronchial asthma and chronic cough (bronchitis and bronchiectasis etc.)
according to the above mentioned chest physicians and they told me that
goat’s milk is never prescribed to their public sector and private
sector patients when they are admitted to hospitals. When I come across
cardiac patients complicated by bronchial asthma and other respiratory
problems. I usually prescribe drugs such as bronchodilators, inhalers
and antibiotics if and when indicated and if there is no significant
improvement. I always refer these patients to chest physicians and
request them to take over for management of the pulmonary problems and
take over for follow-up. To date I have not yet met any physician who
has “experimented” using goat’s milk for pulmonary problems, such as
bronchial asthma (COPD) chronic bronchitis, emphysema or bronchiectasis. I contacted two very highly qualified and highly experienced chest
physicians who have treated thousands of patients suffering from chronic
cough and asthma (bronchial asthma) in Colombo for more than 35 years.
They told me that “you can never cure or bring permanent relief to
patients with chronic cough and asthma by using goat’s milk” and that
“no physician ever treats asthma using goats milk”. The Sri lankan
Government spends millions of rupees annually importing drugs to control
bronchial asthma and chronic cough (bronchitis and bronchiectasis etc.)
according to the above mentioned chest physicians and they told me that
goat’s milk is never prescribed to their public sector and private
sector patients when they are admitted to hospitals. When I come across
cardiac patients complicated by bronchial asthma and other respiratory
problems. I usually prescribe drugs such as bronchodilators, inhalers
and antibiotics if and when indicated and if there is no significant
improvement. I always refer these patients to chest physicians and
request them to take over for management of the pulmonary problems and
take over for follow-up. To date I have not yet met any physician who
has “experimented” using goat’s milk for pulmonary problems, such as
bronchial asthma (COPD) chronic bronchitis, emphysema or bronchiectasis.
Use of goats milk in the cure of eczema
I would be very grateful to any reader who could quote any scientific
evidence (from a recognised medical book or medical journal) to prove
that goat’s milk could permanently cure chronic cough or asthma.
I contacted two highly experienced dermatologists (skin specialists
who are also qualified in allergy) who had served the National Hospital,
Colombo for more than 25 years as dermatologists, as to whether goat’s
milk can cure eczema and urticaria. They told me that goats milk cannot
cure eczema or urticaria as far as they are aware and that there are
many folk tales about goat’s milk among some Sri Lankans.
I contacted a very well-known Professor of Medicine attached to the
Faculty of Medicine, Peradeniya, who informed me over the phone that
goat’s milk is not superior to cow’s milk and that goat’s milk cannot be
used to cure chronic cough, asthma, eczema or urticaria as far as he is
aware.
There are thousands of patients suffering from eczema and urticaria
attending our hospital clinics and BP should encourage a medial person
to do some research with a view to prove that goat’s milk is useful in
the treatment of eczema and urticaria. I am sure, if any Sri Lankan can
scientifically prove to the medial community that goat’s milk can bring
permanent relief to patients suffering from asthma, chronic cough,
eczema and urticaria, that person may receive the Noble Prize in
Medicine.
I am sure BP must have been misled by some non-medical person as
regards the usefulness of goat’s milk. According to all the books on
Nutrition I referred up, there is very little difference between cow’s
milk and goat’s milk. The latter has hardly any carotene, less vitamin
B12 and less iron. Some infants reared on goat’s milk develop anaemia
(due to B12 deficiency plus iron deficiency) referred to as “goat’s milk
anaemia” according to (late) Prof. T.W. Wickramanayake who had made the
biggest contribution to nutrition in Sri Lanka.
Milk allergy
Cow’s milk causes more allergic reactions than goat’s milk during
infancy. Cow’s milk contains more than 40 proteins that can cause
allergy if raw cow’s milk is drunk. Some of the above proteins are
inactivated by heating and cow’s milk allergy occurs in one to three
percent of infants in USA. According to a paediatric colleague of mine,
for cow’s milk allergy best milk is breast milk. In case of mothers who
do not like to breast-feed their children, and in case of those who
cannot secrete sufficient amount of breast milk, they can switch onto
soya based formal cow’s milk allergy is not a problem in children over
the age of three years.
I am sure that by now BP will agree with me that “A little learning
is a dangerous thing”.
D.P. Atukorale,
Colombo 7
|


















