 |
 |
| Sunday, 5 September 2004 |
| Features |
| News Business Features Editorial
|
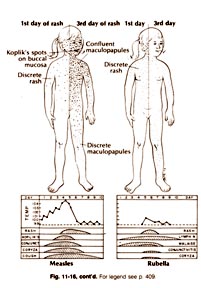
A rash, red eyes, fever? : You could be having Measles
Measles (rubeola), and German Measles are common infectious childhood disease. Dr. Panduka Karunanayaka, Senior Lecturer in Medicine at the Colombo Medical Faculty spoke to Carol Aloysius about the life threatening complications of both these diseases and how they can be prevented. Q: There are many myths surrounding Measles and Rubella. Can you tell us how exactly these diseases are spread? A: Measles (rubeola) is an infection caused by the measles virus which enters the body through the respiratory tract. Rubella is also an infection that is caused by the Rubella Virus through the respiratory tract. On entering the body, the virus starts multiplying and produce thousands of viruses and after a few days it causes the illness. Q: Let's talk about Measles first. How long does it take for the infective virus to develop into measles? A: About two weeks. This is called the incubation period. Q: How does this illness start? A: First with a runny nose that could be mistaken for a common cold. Then fever which can sometimes be as high as 104 -106 degrees F. The patient can also have a runny nose, develop body aches and pains, loss of appetite, vomiting, develop a cough, have bouts of diarrhoea (occasionally with blood and mucus). He/she can also get redness of the eyes with tearing and redness inside of the cheeks and throat. Q: When does the measles rash appear? What do you call this rash? A: From about the third or fourth day or even earlier. We call this rash the Maculopapular rash. You get tiny pin head spots and bumps on the skin. It is a very characteristic rash which can easily be diagnosed. Q: Where does this rash usually appear? A: On the face, then the chest, trunk and limbs. It disappears within seven days, after which the fever will also subside. Q: What is the most infectious period when another person can easily 'catch' this disease from a patient? A: From about two days before the fever to the time the rash disappears. Q: Are there any complications from this disease? A: Most patients get well within a week and there are no complications. But particularly among malnourished children, there can be serious complications. Q: Such as? A: Pneumonia, diarrhoea, encephalitis (brain fever). It can also re-activate healed TB of the lungs. If the chest infection is not properly treated it can lead to a chronic chest infection called bronchitis. Some develop a bacterial infection of the eyes, which if not properly treated can cause blindness of middle ear infections leading to deafness. Rarely, it can cause hepatitis myocadiditis. Q: What is the treatment for Measles? Are there any drugs?. A: There is no special drug that kills the Measles Virus. The treatment is mostly supportive treatment, starting by treating the fever and relieving the symptoms. Make sure that you give the patient proper nourishment and preventing complications. As the patient's appetite is generally poor, give small amounts of food and fluids (milk and soups). Consult a doctor if there is difficulty in breathing or persistent vomiting and diarrhoea. Protect the patient's eyes from strong glare and lights. Q: Tell us about Rubella. Are the symptoms similar to measles? A: Unlike in the case of Measles, there is only mild fever for about 2-3 days and a rash like Measles. But less intense and lasting for a shorter period of about 2-3 days. Usually there is an enlargement of the lymph glands (about the size of a seed of orange at the back of the head and neck. Q: What are the complications of getting this disease? A: Complications to the patient are rare. It may lead to arthritis and in very rare cases encephalitis, hepatitis or bleeding into the skin and mucus membranes. The serious repercussions of this disease are mostly felt by pregnant mothers. Q: Why? A: It can cause several life threatening complications to the foetus (unborn child), especially if the mother contracts the disease in the first twenty weeks of pregnancy, when the baby is just developing. Q: What sort of complications? A: Growth retardation, microcephaly (i.e. brain growth will be curtailed and the brain will be small and abnormal), heart diseases like atrial syndrome (hole in the heart) can also develop, eye problems - from cataract to retina - the whole eye can be affected. Hepatitis and bone skeletal lesions are also common. We call this whole spectrum of diseases Congenital Rubella Syndrome (CRS). Q: How do you treat this disease? A: Like Measles, Rubella cannot be treated with antibiotics as it is caused by a virus. Treatment will be mostly supportive unless there are complications and you have to then treat the complications. Q: Both these illnesses are preventable aren't they? How can one avoid getting either of them? A: By immunising your child with the MR (Measles Rubella) vaccine which is freely available under our Expanded Immunisation Program. We will be conducting a 2nd Measles catch-up immunisation program next month for those who have never been immunised, as to give them a second chance. Q: When does it begin? A: Phase II of the MR catch-up program will begin on September 11 and
12. We urge all those in the age group 16-20 years to receive this
vaccination which will be given on an islandwide basis. Women and heart attacks by Dr. D. P. Atukorale Coronary heart disease (CHD) is the leading cause of death both in women and men. Although the number of deaths due to CHD has declined in men over the last decade, it has actually increased in women. This is because obesity, metabolic syndrome and diabetes disproportionately affect women compared to men, says Dr. D. P. ATUKORALE. CHD in women is different from CHD in men and is a different disease. In females the clinical manifestations of CHD such as angina and dyspnoea (breathlessness) appear approximately 10 or more years later than men. Although women have more symptoms due to CHD than men, coronary angiographic evidence of CHD is significantly lower in women. Sensitivity and especifically of stress testing (exercise ECG) which predicts CHD, is very much lower in women compared to men. Women ultimately have poor outcome than men when they get heart attacks (myocardial infarction). Female pattern of 'angina'and ischaemia related symptoms such as dyspnoea are quite different from those of men. When females get symptoms of coronary artery obstruction such as severe angina, blackouts (due to heart block) and heart failure, they have worse outcome than men. Mortality rates of Coronary Artery Bypass Surgery (CABG) in women is approximately twice that observed in men. For a women under 65 years of age who have myocardia infarct (heart attack) the mortality rate is approximately twice that of men. Overall, the one year mortality rate for women with heart attacks is about 1.5 times the rate for men. For heart failure patients of all ages, the annual incidence rate for women is about twice that of men. In the SOLVED registry, at a one year follow-up, women had higher rates of all adverse outcome rates combined (such as angina, heart attacks and heart failure) compared to men. Why do women suffer from more adverse effects of heart attacks than men? Is it that women have an incomplete understanding of the disease or is it that women have more comorbidities such as obesity, diabetes, hypertension and increased age? Or is it that CHD in women is a quite different disease with more prominent microvascular component or is it that there is a bias in patient care pattern? In the INVEST trial which involved 22,576 CHD patients with hypertension. two drugs (verapamil and atenolol) were tried and 50 per cent of the patients were women. Women had higher systolic Blood Pressure (B.P.) than men and women showed a lower percentage of B.P. control. When the cohort was restricted to 10,000 patients with prior Myocardial
Infarction (MI) or CABG, adverse outcome rates were higher in women. The
rates for heart attacks and strokes were higher in women. Smells of nostalgia Smells can be a powerful trigger of significant memories - but can memories trigger the sense of smell, and what does this imply for the way memories are stored? A study of the smell gateway in the brain carried out at University College London (UCL) has found that the memory of an event is scattered across sensory parts of the brain. By reversing a premise made famous in Marcel Proust's book 'Remembrance Of Things Past,' UCL researchers established that the memory of an event is held in areas of the brain such as the hippocampus as well as in the olfactory cortex - the smell gateway of the brain. In Proust's story, protagonist Charles Swann is mentally transported back to his childhood when the smell of a biscuit dipped in tea triggers memories from his past. Dr. Jay Gottfried and colleagues at UCL's Institute of Neurology set up an experiment to establish whether this mechanism could be reversed, that is whether memories could reawaken the smell-sensitive regions of the brain. The study has been published in the science journal Neuron. A group of volunteers were asked to create stories or links between pictures of objects and various different smells. When the volunteers were later shown pictures of the same objects, their piriform (olfactory) cortex was reactivated although the smell was no longer present. Dr. Jay Gottfried said: "Our study suggests that, rather than clumping together the sights, sounds and smells of a memory into one bit of the brain, the memory is distributed across different areas and can be re-awakened through just one of our sensory channels. This mechanism would allow human beings more flexibility in retrieving their memories." "For example, let's say you spent an enjoyable evening in a nice restaurant and ate a delicious steak. Now, if the memory of this evening was packaged into a single area of the brain, then major aspects of the original evening might have to be recreated to reactivate the memory successfully. "But if the individual aspects of the evening, such as the music playing in the restaurant, the candles on the table and the taste of the steak were stored in different sensory parts of brain, then the whole memory could come back to you through just one of your senses being re-awakened," added Dr. Gottfried. "In an extreme case such as a survival situation, by creating memory associations you would learn to anticipate the pounce of a predator from a number of sensory cues - a pattern of footprints in the sand, rustling of a bush, or a musky scent in the wind - even if you couldn't see it," he said."Advertising relies on the fact that memories are a set of associations rather than unitary chunks - where a picture of woman drinking a cocktail on a beach can stir up your own holiday memories, even if the only similarity between the image and your memory is the sun hat she is wearing. "That sun hat can set off your own memories of feeling the sand between your toes, hearing the crash of waves, and smelling the pungent aroma of seaweed," added Dr. Gottfried. London Press Service Burning sensation in the stomach by Dr. Sampath R. Nanayakkara Q: I have been suffering from a stomach problem for sometime. I entered
university and began missing meals or taking them late. I get What is this condition. How can I be cured of it? Anxious, Wellawatte. A: You are suffering from a condition common to most of the young and middle aged today. Burning sensation of the stomach could be due to many causes. Gastritis is one of the causes, 'ulcers' of the stomach duodenum (first part of the small intestine) and lower end of the oesophagus (i.e. Gullet), the tube which conveys food from the back of the throat to the stomach, Reflux Oesophagitris, and Hiatus Hernia, and very rarely cancer of the stomach and pancreatic disorders are other causes. Apart from these, a high percentage is Psychogenic in origin. A fair number of sufferers who come under this group go on without proper diagnosis, taking antacid tablets on their own (self medication). Only psychological intervention can cure them permanently. Let me explain in the conditions I have mentioned: Gastritis - Means irritation of the inner wall of the stomach, most commonly caused by Aspirin and other drugs used to control pain and arthritis, and alcohol. Recent research has found a Bacteria living in the stomach itself as cause. 'Ulcers' - are gaps in the lining of the stomach wall which allows the acid juice to attack the underlying tissues, and gradually erode them. 'Mental Stress' - is one of the commonest. Endoscopy is the best method to diagnose. Avoiding substances such as ulcer causing drugs, tobacco, alcohol and taking ulcer healing drugs under medical supervision is the available treatment. Reflux Oesophagritis is the back flow of stomach contents mostly the acid in to the oesophagus causing burning and eroding of its lining. Common in middle aged and elderly women. Obesity (overweight) is one of the obvious causes. Heartburn - is the characteristic symptom in this condition. It is a burning type of pain felt behind your breast bone, brought on by bending, lifting or straining. Patient may be kept awaken at night, lying down, sitting up or by taking some food. The pain may mimic Heart attack or angina.Dietary manipulation is very important to minimise the reflux (or backflow). Small and frequent meals are better than large meals. Milk and dairy products (contains large amount of fat) and fatty foods should should be avoided as they tend to delay emptying of stomach contents.Stooping from the waist is to be avoided. Sleep with the head of the bed slightly elevated. Weight reduction is essential in overweight patients. Smoking should be completely given up. Do not consume any medicine without medical advice. Take all tablets with a large amount of water while sitting or standing. |
|
News | Business | Features
| Editorial | Security Produced by Lake House |

 a burning
sensation in the stomach but doctors say it is not gastritis but some
other condition similar to it. I have been advised against taking milk and
cheese.
a burning
sensation in the stomach but doctors say it is not gastritis but some
other condition similar to it. I have been advised against taking milk and
cheese.



