|

National Breastfeeding Week
August 1 to 4:
Breastfeeding brings the best benefits
By Nilma Dole
Breastfeed points
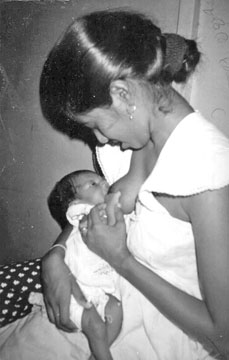
There are three important ways to hold your baby. The cradle
position is popular where you put your baby’s head on the side of
your arm. Then support your baby’s back and bottom with your arm and
hand like a cradle and your baby will now be lying sideways with
baby’s face to your breast. The football position consists of
tucking your baby under your arm like a football resting on your
hand. Support your baby’s body with your forearm. This may be a good
position if you’re recovering from a caesarean section or if your
baby is very small. You can also lie on your side with your baby
facing you.
?The signs that your baby is getting enough milk is that the
baby acts satisfied after each feeding, gains weight constantly
after the first three to seven days after birth, has about six to
eight wet nappies a day, has about two to five or more stools a day
at first and then may have two or less a day.
? Feed your baby as often as he or she wants to be fed as this
may be eight to 12 times a day or more. How often your baby wants to
feed may change over time as he or she goes through growth spurts.
Growth spurts occur at about 2 weeks and six weeks of age and again
at about three months and six months of age.
? Let your baby nurse until he or she is satisfied. This may
be for about 15 minutes to 20 minutes at each breast. Try to have
your baby nurse from both breasts at each feeding. The box lists the
signs to watch for so you’ll know your baby is getting enough milk.
If you’re nursing fewer than eight times a day, be especially aware
of these signs.
Courtesy : www.babycenter.com
Sri Lanka is a leader in promoting breastfeeding awareness not only
within the region but outside as well, said UNICEF Country
Representative, Reza Hossaini at an event to mark National Breastfeeding
Week at the Castle Hospital.
Even though Sri Lanka has been maintaining high figures in
breastfeeding statistics, it is imperative that these figures are
maintained. He said: “Sri Lanka should be proud of achieving MDGs
(Millennium Development Goals) ahead of others in the region but this
does not mean they should take it for granted but keep working at these
figures.”
It will not only be the Government’s role in advocating breastfeeding
but primary health care workers to pregnant mothers too should be
educated on the importance on breastfeeding.
In times of modernisation where there are plenty of career-oriented
women, there needs to be more emphasis on breastfeeding and maternity
leave to suit the working lifestyles. Today, women are sometimes the
sole breadwinners so it is important for companies to recruit women
based on their skills and not on whether they are a burden to the
company for taking maternity leave.
“What is important is that Sri Lankan mothers should know that
breastfeeding is compulsory for six months from the time of the birth of
their child and it is vital that we advocate a good strategy in order to
offer working mothers the benefit of a maternity leave or nursing
breaks,” said Dr. Deepthi Perera of the Family Health Bureau.
She said that it is a benefit for a company where a woman will take
paid maternity leave to breastfeed which will save an immense cost
later. “Rather than taking leave to care for a child, a woman should
take her allocated maternity leave. This is a small price to pay to
ensure that they bring up a healthy child,” she said.
Moreover, Sri Lanka was the first to raise the importance of
breastfeeding as early as the 1970s and it has been in the news ever
since. Today, the Western world now only realises the importance of
breastfeeding after bottlefeeding their babies for several years due to
modernising too quickly.
It is apparent that the health benefits of breastfeeding is high
especially when the child grows older. “It is known that breastfeeding
for as much as one year can increase the immunity of a child and there
is the less chance of the child becoming obese or having juvenile
diabetes,” said Dr. Perera.
According to the doctor, breastfeeding contains antibodies in the
form of colostrum which helps the baby fight diseases which is vital for
not only physical development but mental development too.
“The relationship between baby and mother is more and there is mental
satisfaction when the child feels close to their mother,” she said.
Sri Lanka’s impressive maternal mortality rates where there are
hardly any maternal deaths in childbirth is a good boost to taking
breastfeeding awareness to the next level.
However, while the topic of maternal nutrition is addressed,
malnutrition in children tends to be common after six months because
mothers do not know what to give the child to eat and how to train the
child to eat.
Senior Consultant at UNICEF and government medical doctor, Dr.
Deepika Attygalle said that semi-solids should be given at the early age
as opposed to the liquid food such as porridge or mashed rice.
“Then the child will use their teeth and gums to start to eat. By the
time they reach the age of two, adult food can be given because the
child needs nutrition more than milk,” she said. Dr. Attygalle said that
the problem of malnutrition is not because of lack of food but lack of
giving the right food to the child.
“As medical professionals, we are always glad to assist would-be
mothers so please be careful of taking other people’s advice especially
those who aren’t qualified.
"As doctors we know best and it’s our duty to educate our mothers not
only on breastfeeding but also proper nutrition,” she said.
Speaking at the event was Deputy Health Minister who said, “As a son,
I’ve valued my mother and can say that I’ve achieved success because of
having mother’s milk when I was born.
"I hope this trend continues because it’s not just for the government
to spread awareness but mothers should be educated and ask for advice
from those who know because their child’s health is at stake,” he said.
Mental illness and the stigma associated with it
The stigma that is so deeply attached to mental illness has caused
many authorities in the psychiatric and psychological field to believe
that it has become institutional. One of the troubling aspects of the
stigma is that a large number of people suffering from symptoms of
mental illness do not seek any assistance – despite the availability of
effective treatment – because they are embarrassed, shy or concerned
about what others might think.
 Many don’t share their thoughts or feelings even with close friends
due to these aspects. Many don’t share their thoughts or feelings even with close friends
due to these aspects.
Those who do seek help sometimes find their own self-image eroded by
what’s known as self-stigma, internalizing all these negative
perception.
Most of the patients say they feel a stigma when they are first
diagnosed as having a mental illness. Most say that it is a big blow to
their self-esteem, because then they seen them in that light. And as the
treatment continued, their families too begin it see them in that light
– it began to influence the way they looked at them.
Some psychiatrists and psychologists say that the stigma extends to
primary healthcare.
They say that they had patients whose valid complaints of physical
ailments were ignored once the mental health history was disclosed.
For decades psychiatrists and psychologists have been trying to
eliminate this misconception – to get society to look past this label to
reduce discrimination against people suffering from mental illness. For
those struggling with mental disorders the stigma attached to it is
indeed a beast.
Research has shown that prejudice and discrimination against those
with mental illness can cause more problems than the disorders
themselves.
For example there is clear evidence that finding a partner for a
person identified with mental illness is a difficult task, landlords
won’t rent out to people with mental illness, employers won’t hire then,
police will over-respond and the media will misrepresent.
In fact, analyses of newspaper content in many countries show a clear
pattern of such misrepresentation.
Stories linking mental illness with violence are given more
prominence, more space, and more emphasis than stories about violence
where the suspect did not have a mental disorder.
The overall impression left by such coverage is that people with
mental illness are dangerous. Despite the fact that people who do not
have a mental disorder commit more than 95% of violence in the
community.
The ‘axe-wielding psycho’ is just one of numerous commonly held myths
about mental ill health.
Many still believe that ‘once crazy, always crazy’, despite the fact
that the majority of people with mental disorders recover. Most of the
people cling to the misconception that people with mental disorders are
lazy unpredictable and unreliable.
There is no powerful mental health lobby. Because of this, funding
for mental health programs and research is always substandard – when you
compare with other physical illness funding for mental illness despite
the vast number of people being affected is very poor.
In Sri Lanka, funding for mental health programs has been minimal for
a long time.
For example for research on mental health – the funds allocated is
less than 1% of the population – when there is 25% of the population
that will develop mental illness.
Dr. R.A.R. Perera
Local efforts can stem increasing unnecessary Caesarean sections
Caesarean section rates are steadily increasing globally.
Requiring two doctors to agree that a Caesarean section is the best
way to deliver a baby, rather than just needing one opinion, providing
internal feedback to doctors on the number of operations performed and
seeking support from local opinion leaders may reduce the use of this
procedure.
 For low-risk pregnancies, nurse-led relaxation classes for women with
a fear or anxiety of childbirth and birth preparation classes for
mothers may decrease Caesarean sections. For low-risk pregnancies, nurse-led relaxation classes for women with
a fear or anxiety of childbirth and birth preparation classes for
mothers may decrease Caesarean sections.
On the other hand, providing prenatal education and support programs,
computer patient decision-aids, decision-aid booklets and intensive
group therapy to women have not been shown to decrease Caesarean
sections effectively.
Likewise, insurance reform, legislative changes, external feedback to
doctors on their performance and training of public health nurses to
provide mode of delivery information in childbirth classes do not
decrease Caesarean section rates.
These were the findings of a systematic review carried out by
researchers in Thailand and Australia and published in The Cochrane
Library.
“Around the world more and more women are opting to deliver their
babies by a Caesarean section rather than have the discomfort and
perceived greater risk of a standard vaginal delivery,” says study
leader Suthit Khunpradit, who works in the department of Obstetrics and
Gynaecology at Lamphun Hospital, in Thailand.
He points out that while reported Caesarean section rates vary,
studies have shown that in England, Scotland, Norway, Finland, Sweden
and Denmark Caesarean section rates rose from around 4 to 5% in 1970 to
20% to 22% in 2001.
Furthermore, in 1997 up to 40% of women in Chile opted for a
Caesarean section and current figures show that 46.2% of deliveries in
China are by Caesarean section.
“In 1985 an expert panel of the World Health Organisation suggested
that you could expect up to 15% of women to benefit from a Caesarean
section, but if more were having them, then many were unnecessary,” says
Khunpradit.
While it can be a life-saving procedure for both the mother and the
unborn child, Caesarean sections are also used in situations when
neither the mother nor the unborn child has a greater risk of
complications than the rest of the peripartum population. Caesarean
section itself has risks, including maternal infections, haemorrhage,
transfusion, other organ injury, anaesthetic complications and
psychological complications.
“In some settings, maternal mortality associated with Caesarean
section has been reported to be two to four times greater than that
associated with vaginal birth,” says Khunpradit.
“There is a clear need to halt the escalating use of Caesarean
sections, and from the studies published so far the strategies that had
clearest evidence of reducing the proportion Caesarean sections were
those that focused on the clinicians,” says Khunpradit. He believes
there is clear need for further studies that get higher quality evidence
about interventions that could help women see whether a Caesarean really
is the best option or whether a natural birth would be better.
Sources: Wiley-Blackwell, AlphaGalileo Foundation.
Inherited risk greater for heart attacks than for strokes
People are significantly more likely to inherit a predisposition to
heart attack than to stroke, according to research reported in
Circulation: Cardiovascular Genetics, an American Heart Association
journal. The study results have implications for better understanding
the genetics of stroke and suggest the need for separate risk assessment
models for the two conditions.
“We found that the association between one of your parents having a
heart attack and you having a heart attack was a lot stronger than the
association between your parent having a stroke and you having a
stroke,” said professor of clinical neurology at Oxford University in
England.
“That suggests the susceptibility to stroke is less strongly
inherited than the susceptibility to heart attack.”A second analysis,
which included patients’ siblings as well as parents, yielded the same
result: Family history proved a stronger risk predictor for heart attack
than for stroke. Rothwell and his colleagues conducted the study to
clarify and confirm evidence suggesting a great difference in genetic
predisposition between heart attacks and strokes.
“We had found previously that much of the heritability of stroke is
related to the genetics of high blood pressure, which doesn’t seem to be
the case for heart attack,” Rothwell said. Hypertension appears to be
closely related with stroke rather than heart attack, which is why a
family history of hypertension is related to a higher risk of stroke.
In the report, all patients were enrolled in the ongoing Oxford
Vascular Study. OXVASC, as the study is known, that began in 2002 to
study strokes, heart attacks and other acute vascular events in a part
of Oxfordshire County where more than 91,000 people are served by one
hospital. Previous analyses in the same population conducted by lead
author, Amitava Banerjee MPH PhD, have shown the particular importance
of family history in mother-daughter transmission in both heart attacks
and stroke. “Family history of heart attacks and family history of
strokes have rarely been studied in the same population,” Banerjee said.
The researchers used data from 906 patients (604 men) with acute heart
ailments and 1,015 patients (484 men) who suffered acute cerebral
events. Among the study’s findings:
*In the heart patients, 30 percent had one parent who’d had a heart
attack, 21 percent had at least one sibling who had suffered a heart
attack. Seven percent had two or more siblings who had heart attacks and
5 percent had two parents with heart attack.
*Among the patients with a stroke or transient ischemic attacks (TIAs,
often called a mini-strokes or warning strokes), 21 percent had one
parent who had a stroke, and 2 percent had two parents with stroke.
Eight percent had at least one sibling with a stroke and 14 percent
had at least two siblings with stroke.
*The risk of a sibling developing acute heart problems was similar
for those with heart attack or stroke.
*The risk for an acute cardiac event was six times greater if both
parents had suffered a heart attack and one-and-a-half times greater if
one parent had a heart attack. In contrast, the likelihood of stroke did
not change significantly with parents’ stroke history. The findings, if
confirmed by additional studies, hold two significant implications,
Rothwell said.
“First, the way physicians predict the odds of a healthy person
suffering a heart attack or stroke needs refining,” he said.“Currently,
most risk models lump a patient’s family history of stroke and heart
attack together. We probably should model family history of stroke and
heart attack separately in the future.”
Source: Maggie Francis American Heart Association
|














")