
Goiter: Cosmetically unpleasant but treatable
by Dr. Melanie Amarasooriya
It grows slowly, into a lump in the front of the neck. It seems to
move up and down when you swallow anything. And we call it goiter.
Whenever we hear the term 'goiter' or enlarged thyroid gland, iodine
deficiency is the cause that runs through our minds.
"Although it is the commonest preventable cause of goiter, it is not
the only one", says Dr. Nalitha Wijesundera, a Consultant Surgeon, at
Karapitiya Teaching Hospital.
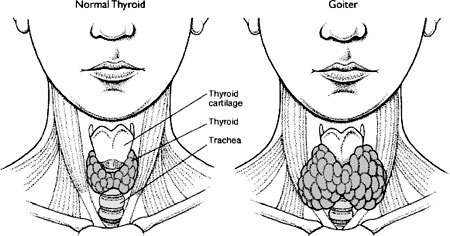
Goiter means simply the enlargement of the thyroid gland. The thyroid
is a butterfly shaped structure located in the front of the neck, just
below the adam's apple, covered with the thin muscles of the neck.
It produces hormones, mainly thyroxin, a vital chemical to maintain
the normal functions of the body. The normal gland is small and not
visible to the exterior.
However the gland can get enlarged due to variety of reasons and this
enlargement is called "goiter."
The process could be normal, when the thyroid enlarges due to normal
processes in the body like pregnancy and puberty. During these periods
the gland has to work more, so that the cells multiply and the gland
becomes larger in size, retaining the normal shape. However, this
resolves when the period of increased demand is over.
Sometimes, goiter occurs because of lack of production of thyroid
hormone.
 It is fairly common in our country. In this instance, when the output
from the thyroid gland is low, due to any particular reason, the
pituitary gland in the brain tries to send more and more chemical
signals to stimulate the thyroid to increase its hormone production. The
result is, the gland getting enlarged gradually in response to this
stimulation, but the production of the hormone remains low. It is fairly common in our country. In this instance, when the output
from the thyroid gland is low, due to any particular reason, the
pituitary gland in the brain tries to send more and more chemical
signals to stimulate the thyroid to increase its hormone production. The
result is, the gland getting enlarged gradually in response to this
stimulation, but the production of the hormone remains low.
The causes for lack of hormone production by the gland are numerous.
If the hormone production is low due to lack of iodine in food,
increased iodine intake would reverse this procedure and shrink the
gland in the initial stage.
But if there is an intrinsic problem in the gland, making it
difficult to produce the necessary amount of thyroxin, iodine would not
solve the problem. So the next step is to resort to thyroxin tablets,
i.e. to take the thyroxin hormone as a tablet.
This type of thyroid enlargement, occurring due to hormone deficiency
is called "hypothyroid goiter" meaning the level of thyroxin in the body
is less than the normal.
This could occur from birth, but not very common.
Commoner form of hypothyroid goiters occurs in the middle age, in
women, which is not diagnosed until late. This is because the symptoms
of these conditions can sometimes be confused with the normal complaints
with aging.
To add to the problem their thyroid glands may not be very large, not
disfiguring to the extent to seek medical advice. The only symptoms they
have are the features of hypothyroidism or lack of thyroxin hormone.
Hypothyroidism
Lethargy weight gain without a significant change in appetite
Constipation
Dry skin
Thin hair
Mental slowness
Hoarse voice
Cold intolerance
Low pulse rate
When the goiter is long standing, it undergoes certain permanent
changes so that after a particular point the goiter does not shrink with
treatment. In fact it feels nodular or having numerous small lumps in
the gland like.
You may also feel one small lump when there are other smaller ones
which can not be felt.
At this point if the goiter is large, causing cosmetic problems,
difficulty in breathing due to pressure on the respiratory passage or
difficulty in swallowing, it needs surgical intervention.
The option is to surgically remove the thyroid gland.
The other entity with thyroid gland is hyperthyroidism or excessive
production of thyroid hormones. This is mainly due to abnormal proteins
unduly stimulating the gland, to produce excessive hormones. This gives
rise to "thyrotoxicosis" with the following features.
Hyperthyroidism
Irritability, Excessive sweating, Diarrhoea, Loss of weight,
Increased appetite, Tremor, Warm, Sweaty fingertips, Increased pulse
rate.
The usual picture in hyperthyroidism settles in about two years. The
objective of the treatment is to reduce symptoms until the gland
spontaneously becomes normal.
Therefore, anti thyroid medication are prescribed for about one and
half years. However, in certain instances radio active substances can be
used to shrink the gland and lessen the production of hormone. Also,
once the patient is stable on medication, surgical removal of the gland
could also be performed safely so that further such episodes are
prevented.
In addition to alterations in the hormonal levels causing a disease
process, there are other causes which lead to enlargement of the gland,
namely malignancy, or cancers in the thyroid gland.
Although cancers are not as common as harmless enlargement of the
gland, thyroid cancer is not a rare one. In fact the commoner varieties
of thyroid cancer are seen among young people.
It usually starts as a single nodule in the front of the neck. This
nodule may be hard, but painless. There may be accompanying nodules on
either side of the neck due to enlargement of lymph nodes.
Thus, whenever there is a lump which developed recently in the front
of the neck, it is always advisable to seek medical advice. Recent
change in the voice, occurring with a lump also suggests that you need
to see a doctor without delay.
However, most of the patients with thyroid cancers do not show
symptoms of altered hormone levels.
Their hormone levels are usually normal.
A doctor, after examining the neck can tell you whether the lump
arises from the thyroid gland and whether further investigations are
necessary. Depending on the findings of examination, you may need to
asses the function of the thyroid gland, by blood tests which measure
the hormone levels, an ultrasound scan of the neck and fine needle
aspiration cytology or FNAC.
In FNAC a small needle is used to obtain few cells from the lump to
be examined under the microscope. If these investigations point towards
malignancy, you will need surgery to remove whole or part of the gland.
Yet the conclusion of cancer is done only after examining the
surgically removed gland.
So even if you undergo removal of part of thyroid gland for a
suspected cancer, the final report could come as a 'harmless lump'. Thus
thyroid surgery is never synonymous with cancer.
Also if diagnosed early and prompt treatment is given the outcome
with thyroid cancers is good. Majority of The young patients who undergo
surgical removal of the thyroid gland for common varieties of thyroid
cancer can live more or less a normal life.
If the gland is completely removed due to any cause the patient has
to be on lifelong thyroxin hormone therapy.
It does not cause any side effects as the pill only contains a
hormone which is normally found in the body. Also, patients should not
stop the treatment, because thyroxin is a vital hormone to maintain the
functions of the body.
(Information provided by Dr. Nalitha Wijesundera , Consultant
Surgeon, Karapitiya Teaching Hospital)
Boy babies 'worse for depression'
Giving birth to a boy can increase the likelihood of severe postnatal
depression, a study suggests.
 French researchers examined 181 mothers, and found 9% had severe
depression - three-quarters of these had delivered a male child. French researchers examined 181 mothers, and found 9% had severe
depression - three-quarters of these had delivered a male child.
The Journal of Clinical Nursing study suggested earlier poor
relationships with men could be a factor for some.
However, a specialist in the UK said the finding, although
interesting, could be a "statistical quirk".
* The overwhelming finding of the study was the fact that gender
appears to play a significant role in reduced quality of life as well as
an increased chance of severe postnatal depression Professor Claude de
Tychey University of Nancy Postnatal depression is common among new
mothers - the latest study at the University of Nancy found a third of
those taking part were affected to some degree.
The women involved were questioned on several different areas of
their health, including physical fitness, pain and mental and emotional
health.
The researchers, led by Professor Claude de Tychey, found that seven
out of ten women who had given birth to a boy reported a lower quality
of life compared with the average of women who had given birth to a
girl, regardless of whether they had postnatal depression.
Although mothers of girl babies were more likely to have mild
postnatal depression, among the 17 women diagnosed with severe postnatal
depression, 13 had had male babies.
The researchers did not have any evidence of a reason behind this
difference, and called for further research to discover it.
However, although they suggested there might be subtle psychological
differences in the attitudes of new mothers towards boy and girl babies
which might affect their emotional state - particularly if they were
already prone to depression.
They suggested a negative attitude to a son might be a legacy of
unsatisfactory relationships with important male figures in their life,
such as their father, or partner.
Professor de Tychey said: "The overwhelming finding of the study was
the fact that gender appears to play a significant role in reduced
quality of life as well as an increased chance of severe postnatal
depression.
"Women had the same scores regardless of whether the recent birth was
their first or second baby."
However, Dr. Cosmo Hallstrom, a member of the Royal College of
Psychiatrists, said the numbers of women with severe depression were too
low to draw firm conclusions.
He said severe depression results were compromised by the finding
that a majority of the mothers with mild depression were more likely to
have given birth to girls.
He said: "It's an interesting talking point, but I'm not entirely
convinced by this, and would like to see it replicated in larger trials.
"It's probably a statistical quirk."
BBC NEWS
Psychological problems and bowel disorders
by Dr. R. A. R. Perera, Consultant Psychologist
It is generally accepted that no organic cause can be found for many
abdominal pain patients attending medical clinics, even after through
laboratory and clinical investigations.
 These patients are often labelled as suffering from irritable bowel
syndrome. The diagnosis of irritable bowel syndrome is based on the
exclusion of organic disease in a patient complaining of abdominal pain
and a disordered or irregular bowel habit. These patients are often labelled as suffering from irritable bowel
syndrome. The diagnosis of irritable bowel syndrome is based on the
exclusion of organic disease in a patient complaining of abdominal pain
and a disordered or irregular bowel habit.
Patients are often subjected to numerous repetitive investigations,
even including surgery in some cases. The results of these
time-consuming and expensive tests are invariably normal.
Sooner or later the patient's symptoms are ascribed to psychological
causes and labelled as functional. There is a widespread belief that
psychological factors are paramount in the causation of bowel disorders,
although this view has largely arisen on the basis of failure to find
organic abnormalities.
Excessive and uncoordinated segmental contractions of the large bowel
have been reported in patients with irritable bowel disorder. An
abnormal psychological mechanism can cause this disordered function of
the bowel.
The tendency to this disorder may be congenital or acquired.
Sometimes other members of the family might have similar abdominal
pains, which cannot be explained medically.
In Sri Lanka, despite the widespread occurrence of irritable bowel
disorder, and the large number of patients in whom the diagnosis is
made, few formal studies of the psychological aspect of this condition
have been carried out.
There is high incidence of depression, anxiety and marital
difficulties in patients complaining of irritable bowel disorders. The
obsessional personality, with traits such as orderliness, rigidly,
conscientiousness and preoccupation with planing and detail, has been
emphasized in these patients. Such people may have a limited awareness
of their emotional problems, and a limited capacity for emotional
expression.
There is no doubt that emotional states can profoundly affect bowel
function. Irritable bowel disorder is a chronic condition characterized
by relapses and remissions. There is an association between relapses of
this disease and critical life events.
Depression: Changes in appetite and weight are common in depression.
Anorexia and retardation of activities, which is associated in
depression, can cause constipation. Diarrhoea may occur in agitated
patients. Abdominal pain may also be a feature of depression.
Anxiety: The biological accompaniments of anxiety often include
diarrhoea. Muscle tension associated with anxiety may produce abdominal
pain. Morbid preoccupation with bodily function, and especially bowel
function, may be a feature of anxiety states.
Management: It is essential to establish the diagnosis and to carry
out all the investigations necessary for the exclusion of organic
disease at the outset. After that, the approach to the patient should be
holistic, with the emphasis shifting from the somatic to the
psychological.
The treatment therefore does not consist of prescribing either an
antidepressant or a high fibbre diet, but should be adjusted to suit the
circumstances of each individual.
The relationship between the doctor and the patient is especially
important. Patients with irritable bowel disorder often need repeated
opportunities to discuss their symptoms with the doctor. They are quite
likely to have had numerous previous consultations and investigations
elsewhere and to have been told that 'there is nothing wrong'.
This generates feelings of frustration and guilt in the patient and
lack of sympathy in the relatives.
The doctor should accept, and be seen to accept, that the symptoms
are real and not imagined by the patient. Sympathetic supportive
psychotherapy will, in most cases, provide greater insight in to the
background of the symptoms and thus enable the patient to cope better.
Irritable bowel disorder is a chronic relapsing condition, which
extends over many years, sometimes to the childhood. Whatever the
treatment, the condition could last for a long period of time.
Lack of improvement should not lead to discontinuation of treatment.
It may be helpful to interview the spouse or other members of the family
together with the patient, any underlying psychopathology should be
treated.
In Sri Lanka, native treatment offered by the 'vedamahaththaya' is a
popular way of treating irritable bowel disorder. Some times it is an
effective treatment either due to the medications or due to the
'psychotherapy' which is a part of the 'treatment'. |













