|

New techniques in IVF offer… :
Fresh hope for childless couples
By Carol Aloysius
Time was when desperate couples who were unable to have their own
child were forced to adopt a child. Some even resorted to illegal
methods such as kidnapping newly born babies from hospitals, or buying
them from poor mothers. This is because many of them are unaware they
have access to an alternative, safe method. Medical technology has given
them new hope by opting for In-Vitro Fertilisation (IVF), which has up
to date successful results, not just in Sri Lanka, but globally as well.
Infertility physician and Clinical Embryologist Dr HELARUWAN PASAN
KUMARA talks to the Sunday Observer on some of the recent advances in
this speciality.
Excerpts…
|
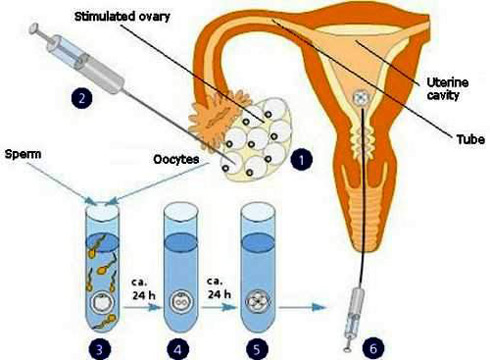
Simplified IVF process |
Q. In-vitro fertilisation (IVF) has become a major technique
for couples who have failed to have a child by other methods. Explain
what IVF means.
A. IVF means fertilisation of a woman's ovum (eggs) and man’s
sperm which takes place outside the body in a specialised lab
environment.
Q. Since infertility is the root cause for using this
technique, what are the reasons that make couples infertile in the first
place? Genetic problems? Birth defects? Accidents? Age of mother and
father? Lack of sperms or limited number of sperms?
A. Infertility is caused by three ways: Women's reproductive
problems, men's sexual problems and idiopathic causes. The main problem
for women is not being able to produce good quality eggs to conceive due
to various reasons such as ovulatory failure, age, genetic issues,
radiation etc. Other than that, fallopian tubal problems, diseases such
as endometriosis and other endocrine problems can also affect women's
fertility.
Q. What about men?
A. In the case of men, their sperm count can be low due to
genetic issues, infections, sperm travelling tubal obstruction, hormonal
imbalances etc. The number, speed and morphology
of the sperm is important for fertilisation. When the clear cause is not
detected for their infertility they fall into the Idiopathic category.
Q. Prior to IVF, do they have other methods to become fertile?
A. Timed intercourse in natural cycle, Intra Uterine
Insemination (IUI), are methods they should try to address the root
cause before they enter into an IVF program.
Q. Are those methods less drastic than IVF? Less harmful to
the mother and unborn child?
A. Yes. IVF is the most invasive method of all. But it is also
the most successful method. Even other methods like IUI can lead to some
side effects. But current methods of new ovulation induction leads to
less harmful IVF cycles.
Q. Describe the IVF procedure. Is it done manually or with
machines?
A. Most of the procedure is done manually. But for freezing of
embryos some centres use machines.
Also latest techniques such as embryoscope are now being used for
ease of the procedure.
Q. Does a couple have to be hospitalised for this procedure?
If so for how long?
A. There is no need to be hospitalised over night. Only
during an egg retrieval procedure, it will be necessary for admission to
hospital for two to three hours.
Hospitalisation is not required even during embryo transfer.
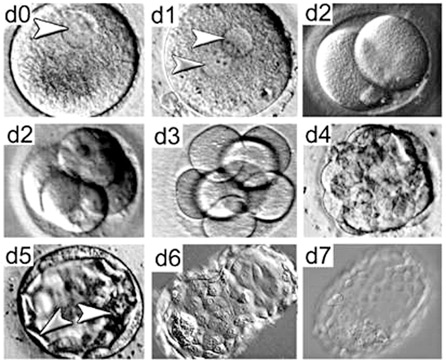
Q. What is an IVF cycle?
A. Firstly using hormones multiple follicles
produced from the woman's ovary.
Then the eggs are retrieved from follicles transvaginally with
minimal invasive methods.
Next, the man’s sperms are collected and from them, the best sperms
are selected. Thereafter, the sperms and eggs are mixed together in
special culture media under special environmental conditions or else
undergo ICSI procedure. The growth of embryo is checked everyday till
day three or five in special culture media. Best embryos are selected
and transferred in to the mother’s womb on day two, three or five with
special hormonal support for the embryos.
Q. What happens to the extra embryos?
A. Extra embryos are frozen for future use. They are stored in
-296 c.
Q. What advice do you give to parents during an IVF cycle?
A. They should not smoke or drink alcohol during and before
procedure.
Doctor should be informed of all medication both partners are using
before and during the procedure. We also advise them to spend a less
stressful lifestyle for more successful results.
Q. What safety measures are there in the lab?
A. All labs are well planned specialised areas. There are
special techniques for quality control and quality assurance of the
labs. There are special guidelines for embryologist to control lab.
Most of the equipment in the labs are to produce environment similar
to the mother’s womb. They should be zero percent infection free. All
embryos grow inside special incubators, so embryo handling is done with
special care.
Q. How do you ensure the quality of the eggs? How do you
decide how many eggs to transfer, once the procedure is over?
A. Quality of eggs depends on the woman's age, stimulation
protocol and manipulation during egg retrieval, and all steps are taken
to control and produce the best quality eggs.
Transferred number of embryos depends on quality of embryos, patients
request and available number of embryos. Usually one or
two embryos are transferred depending on age of embryo.
Q. How long can the eggs be stored? Can sperms be stored from
a dead person?
A. Eggs and embryos can be frozen and kept for about 10 years
or more in specialised conditions. Even a dead person’s eggs can be
frozen for future use. But this has to be done very quickly. Sperms also
can be frozen for future use.
Q. When is the first pregnancy test after the eggs are
inserted?
A. A blood test is done 14 days after the embryo transfer.
Q. What happens if she fails to get pregnant? Can she try
again? For how long?
A. If she has frozen embryos she can transfer them back. Or
she can try again and undergo fresh IVF cycles as many times she wishes
till she produce good quality eggs.
|
Stages of human embryo development |
Q. Is IVF legally allowed for any infertile couple?
A. In Sri Lanka any couple can enter the IVF program. All our
procedures are also done on a confidential basis.
Q. What are the medical ethics involved?
A. Informed written consent is major area. Donor embryos, and
surrogate and sex selection issues are also major areas involving
medical ethics. All donors and surrogate mothers are screened for STDs
specially HIV/AIDS and have to pass the quarantine period before
entering the program.
Q. When was IVF first introduced 1) globally 2) in Sri Lanka?
A. Globally - end of 1970. In Sri Lanka - end of 1990.
Q. What does the procedure cost?
A. Cost is usually around Rupees five lakhs. But this cost
can be reduced to half if they go under an egg sharing program. In
future we plan to reduce the cost more.
Q. Any recent breakthroughs in the techniques used?
A. ICSI (Intracyto Plasmic Sperm injection) is a recent
technique, which enables almost all infertile males to produce babies.
Also new freezing techniques like Vitrification increase the success of
IVF. PGD (Pre Implantation Genetic Diagnosis) ensures more healthy
babies being produced with the best genetic material.
Q. Are they available in Sri Lanka?
A. Yes, we have all new techniques except PGD. Hopefully
this will be available in the near future.
Q. Your advice to couples without children?
A. Couples who have failed with other methods, over a period
of time since marriage, should enter the IVF program quickly for more
successful results, as age is an important factor.
Those with financial problems can discuss an egg sharing procedure
which is less costly.
Polypill increases adherence to post MI treatment
A new polypill increases adherence to treatment following a
myocardial infarction (MI), according to results from the FOCUS Study
presented for the first time at ESC Congress 2014 by principal
investigator Dr Valentin Fuster, director of Mount Sinai Heart in New
York, US (1). The novel treatment regime has the potential to prevent
more patients having a second heart attack.
Dr Fuster said: “Despite continuous advances in all areas of
cardiovascular (CV) medicine, cardiovascular disease (CVD) has steadily
increased in prevalence to become the number one cause of death
worldwide. It is estimated that half of the overall reduction in CVD
mortality observed over the past 20 years in western countries could be
attributed to appropriate use of CV medications for secondary
prevention. But lack of adherence to treatment impedes adequate
secondary prevention and contributes to the CVD pandemic.”
 He continued: “The most important factors responsible for a lack of
adherence to treatment are the complexity of treatment and the daily
number of prescribed pills. He continued: “The most important factors responsible for a lack of
adherence to treatment are the complexity of treatment and the daily
number of prescribed pills.
The idea of using a polypill for CVD prevention has gained increasing
momentum because it could increase adherence and therefore contain the
progression of CVD. A polypill could simplify healthcare delivery,
improve cost-effectiveness, support the comprehensive prescription of
evidence-based cardioprotective drugs, and reach underdeveloped regions
of the world.”
The Fixed-dose Combination Drug for Secondary Cardiovascular
Prevention (FOCUS (2)) study was established to investigate adherence to
secondary prevention medication and test a new polypill.
The study was conducted in two subsequent phases. FOCUS 1 included
post MI patients in a multi-country comprehensive analysis of
socio-economic, comorbidity, and other factors
that determine adherence to CV medications. FOCUS 2 was a randomised
controlled clinical trial testing the effect of a fixed-dose combination
(FDC), the CNIC-FS (3)-FERRER polypill, containing acetylsalicylic acid
(ASA) 100 mg, simvastatin 40 mg and ramipril 2.5, 5 or 10 mg, on
adherence and control of CV risk factors in post MI patients.
FOCUS 1 included 2 118 patients with a history of MI from five
different countries (Spain, Italy, Argentina, Brazil and Paraguay).
The degree of adherence to prescribed medications was calculated
using the Morisky Green Adherence Questionnaire, a self-reported method
with four questions on adherence behaviour.
The researchers found an average baseline adherence level of 45.5
percent.
The researchers also conducted a descriptive analysis of variables
that impede adequate adherence.
They found that patients below 50 years of age, those taking more
than 10 pills, following a complex regimen (i.e. those taking
medications other than orally), current smokers and those with sedentary
lifestyles were significantly more non-adherent.
Dr Fuster said: “Importantly, there was a significant trend towards
more non-adherence with a higher score of depression
(as measured by the PHQ-9 questionnaire). Of the socio demographic
variables, illiteracy level, lower social support and lower percentage
of insurance cover showed significantly lower levels of adherence as
well as those patients being treated by general practitioners (as
opposed to cardiologists) and being treated in a private centre (as
opposed to a public health centre).”
In a stepwise forward regression model, FOCUS 1 found that the risk
of being non-adherent was independently associated with younger age
(under 50 years old), scoring high on the depression scale, and
following a complex (administrations other than oral) treatment.
On the other hand, the odds of being adherent increased with higher
percentage of health insurance coverage, and with optimal levels of
social support.
In FOCUS 2, a total of 695 patients were enrolled from four countries
and followed for a period of nine months. Patients were randomised to
receive either the polypill or the three drugs separately.
Adherence was measured with two methods: self-reported adherence
using the Morisky Green Adherence Questionnaire as well as a direct
method, the pill count.
The results after nine months of follow up are shown in figure 1.
Dr Fuster said: “Patients were more likely to take their medication
to prevent a heart attack when it was given as a polypill, rather than
as three separate pills. We found this using two methods. With the
self-reported questionnaire, 68 percent of patients in the polypill
group took their drugs compared to just 59 percent of patients in the
group assigned to three drugs.
With the pill count, we found that 92 percent of patients in the
polypill group were adherent compared to only 84 percent in the group
assigned to separate drugs.”
- MNT
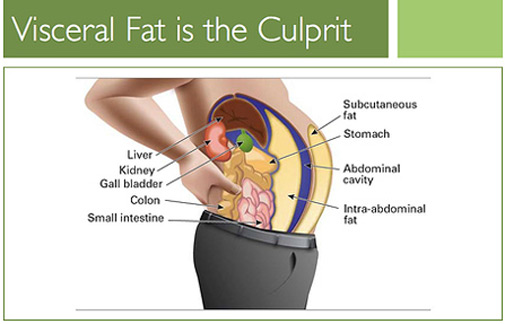
Abdominal fat increases risk of high blood pressure
 People with fat around their abdominal area are at greater risk of
developing hypertension when compared to those with similar body mass
index but fat concentrations elsewhere on the body, according to a study
published in the Journal of the American College of Cardiology. People with fat around their abdominal area are at greater risk of
developing hypertension when compared to those with similar body mass
index but fat concentrations elsewhere on the body, according to a study
published in the Journal of the American College of Cardiology.
Obesity is a known risk factor for hypertension, or high blood
pressure, and it is widely reported that the location of fat on a
person's body can lead to increased risk of other health issues such as
heart disease and cancer. However, the relationship between hypertension
and overall obesity versus site-specific fat accumulation is unclear.
For this study, 903 patients enrolled in the Dallas Heart Study were
followed for an average of seven years to track development of
hypertension. Hypertension was classified as a systolic blood pressure
of greater or equal to 140, diastolic blood pressure of greater or equal
to 90, or initiation of blood pressure medications. Patients also
received imaging of visceral fat, or fat located deep in the abdominal
cavity between the organs; subcutaneous fat, or visible fat located all
over the body; and lower-body fat.“Generally speaking, visceral fat
stores correlate with the ‘apple shape’ as opposed to the ‘pear shape,’
so having centrally located fat when you look in the mirror tends to
correlate with higher levels of fat inside the abdomen,” said senior
author Aslan T. Turer, a cardiologist in Dallas.
- MNT
A Pictorial Journey of Surgery
An unusual exhibition, probably the first of its kind will open to
the public on September 12 - 14, when a long experienced surgeon, Dr
Gamini Goonetilleke shares his portfolio of photographs spanning 33
years, of surgeries he has performed.
Titled A Pictorial Journey of Surgery Through the Lens, he says his
main objective in holding the exhibition, is to educate the public and
inform them of the various surgical techniques now available to them for
different diseases, and to detect early symptoms of diseases such as
breast and bowel cancer. On view will be different types of hernia and
surgery complications, surgery and need for early medical advice on
goitre, latest techniques on removal of gall bladder stones as well as
the terrible consequences of road accidents and drinking alcohol and why
they should be avoided at all costs.
Also on view will be some rare conditions such as Rapunzel syndrome
(eating hair) which too has been successfully treated by him.
The exhibition is open to all while entrance for school children is
free, if accompanied by school authorities.
It will be held at the Auditorium of the College of Surgeons, No 6,
Independence Avenue, Colombo 7 from 9 am to 8 pm on September 12 to 14. |












")


