|

Spinal cord injuries - prevention the key
Total care, a fresh approach to rehabilitation of
victims:
By Carol Aloysius
A surge in alcohol related violence, reckless driving and accidental
falls from great heights have collectively led to a sharp increase in
the number of patients with spinal cord injuries (SCI) in Sri Lanka. It
is estimated that between 1,500 to 2,000 persons are paralysed from SCI
per year. Spinal cord injuries are permanent with victims likely to die
prematurely due to various complications they develop along the way.
Having a non communicable disease, lying in bed for a long time, long
periods of immobility - all these can have their toll on the patient.
 Apart from these physical scars, patients, who are mostly males aged
20 and upwards in the prime of their lives, also suffer psychological
trauma from being isolated from their loved ones, deprived from their
erstwhile positions of breadwinners and head of the family. Society
further isolates them by making them social outcasts. Apart from these physical scars, patients, who are mostly males aged
20 and upwards in the prime of their lives, also suffer psychological
trauma from being isolated from their loved ones, deprived from their
erstwhile positions of breadwinners and head of the family. Society
further isolates them by making them social outcasts.
“Paralysed patients due to a spinal cord injury are a major challenge
for their management, rehabilitation and survival as a whole. The
resultant consequences to the patient, family, society and health care
sector is enormous”, President of the Sri Lanka Spinal Cord Network and
Consultant Orthopaedic Surgeon National Hospital Sri Lanka, Dr NARENDRA
PINTO pointed out at discussion with other experts in the field, held at
the Health Education Bureau last week.
Medical student Dinesh Palipana also gave us his personal experience
on the subject.
Following are excerpts of the discussions...
The speakers first explained that the spinal cord was part of the
central nervous system, and an extension of the brain stem usually 10 mm
- 18” in length. The cord communicates between the brain and the rest of
the body and thus functions primarily in the transmission of neutral
signals between the brain and the rest of the body. It also contained
neutral circuits that could independently control numerous reflexes and
central pattern generators.
“When a spinal cord is damaged or there is a break in the cord, no
message will be able to get through to the brain.” Dr Pinto said. Citing
an example, he said that when we place our hands on a hot iron
accidentally, the message immediately is conveyed to the brain warning
us that it could burn our hands.
However, if a person with a spinal injury places his hand on a
burning hot iron he will not realise he is touching something hot as no
message is conveyed to the brain, and he could burn his hands without
even feeling the heat.
“Spinal cord injuries are permanent. If there is a partial injury we
may be able to minimise the injury to some extent. But if the full spine
is broken, we can't repair it. So the important thing is to PREVENT
these injuries occurring”, he stressed.
However, he added, even though spinal cord injury patients have to
face many obstacles, all is not lost since their brain continues to
work.
“If they use their brain well and intelligently, they can do many
things that non patients can do with the help of their carers”, he
noted.
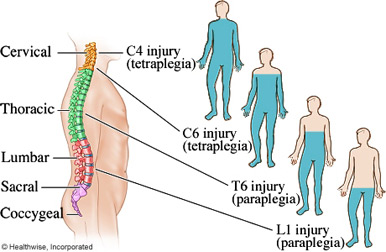
Describing the levels of injury to the spine and the extent of
paralysis, he said that the worst affected were paraplegic patients who
suffered from paralysis in all four limbs.
“They need life long care which affects them, their family, society
and country’, he noted.
Consultant Rhuemotology and rehabilitation, Negombo Hospital, Dr
GUNENDRIKA KASTHURIATNE, in her discussion on ‘Long Term Rehabilitation
of patients with SCI’, summarised the impacts of a spinal cord injury on
the human body. She listed the following as the most common symptoms:
Sudden paralysis of the legs and arms: Loss of sensation in the trunk
and legs: Loss of bladder control: Loss of control in defecating: and
problems with sexual functions.
“Patients with SCI also suffer from pressure ulcers (bed sores) due
to their long period of immobility, from contractions and spasms and
also respiratory (chest) infections leading to pneumonia.
They can also develop urinary tract infection, leg swelling, Deep
Vein thrombosis (DVT), constipation and fractures,” she said.
Another important fall out of the injury, was depression which many
patients suffered from due to their loss of jobs as breadwinners and
inferior dependent role within their families and in society as well as
their sense of social isolation. She said that the goal of the
Rehabilitation Centre at the Ragama Hospital in Negombo was mainly aimed
at reducing the impact of disability in patients and improving their
quality of life and survival.
“It is essentially team work by many people: When a patient is
brought out of the ICU or even when in the ICU, he will need the help of
a multidisciplinary medical team: physiotherapists to improve his body
movements and circulation, occupational therapists, medical doctors,
neurologists, speech therapists to train them to use their vocal cords
and help them breathe properly, plastic surgeons if his injuries have
impaired his face or some other part of the body, opticians if their
eyes are impaired.
Since all of them suffer from stress related disorders due to their
injuries and are depressed, they will need psychologists, social workers
to attend to the immediate needs of their families and sort out their
insurance etc. We work with all of them including their care givers who
need guidance on how to look after the patient", she said. She also
stressed that they required custom made wheel chairs in order to prevent
further injuries.” Any help from the public is welcome”, she said.
"We also have a workshop where we provide them with alternative
occupations they can do in spite of their handicaps,” she said. Director
YEDD, Ministry of Health Dr LAKSHMI KUMARATHILAKE stressed that
Rehabilitation of a disabled person should not be mistaken for buildings
and infrastructure rehabilitation.
It relates to the health of the person who has a disability and the
health impacts that can occur as a result of that disability. Non
communicable diseases such as diabetes which if uncontrolled in a
disabled person could lead to amputation, further aggravating his
disabilities. She noted that for the first time a national policy and
guidelines for rehabilitation services in Sri Lanka had been drafted for
2014/15 and a Disability Steering committee had been set up with multi
stakeholder membership.
National Professional Officer (NCD) WHO Dr LANKA JAYASOORIYA giving
the International Perspective on Spinal Cord Injury said that those at
risk of SCI were mainly young males between 20-29 and those over 70
years.
In females those most at risk were those between 15 -19 and above 60
years.
The causes are Road Traffic Accidents, Falls, Crashes and Violence.
Timely pre-hospital care, quick recognition of suspected SPI, rapid
evaluation of injury and injury management including immobilisation were
vital factors. She further emphasised the need for accessibility for
disabled persons, in schools and public buildings, super markets and on
the roads.
“We should provide a safe and friendly environment for them. We also
need to tell people how to prevent SCI. If injured these patients must
be taught how to survive and lead a quality life despite their
handicaps.”
Facts on SCI
 *Spinal cord injury is a devastating and preventable neurological
injury *Spinal cord injury is a devastating and preventable neurological
injury
* It results in varying degrees of paralysis sensory loss and
sphincter disturbancesloss of control of bladder and bowel) which are
permanent and irreversible.
* Two ways of damaging the cord- Traumatic and non traumatic
Causes
*Domestic and industrial accidents Domestic ( falls from trees ,
ladders / stairs
*Accidents at work - falls from scaffolding, ladders , crash injuries
*Road accidents
*Self harm and criminal assault
*War casualties
*Diseases
* Neuro-degenrative diseases.
Effects
* spinal shock-sudden disability, changes in life pattern Loss of
sensory and motor function below the level of the lesion Complete
immobilityComplete dependence on others Stresses of hospitalization ,
pain and incapacity Uncertain future
Other effects
* Bowel , bladder sexual dysfunction
Male fertility affected
Very high injuries can result in loss of involuntary functions
including ability to breathe necessitating breathing aids, such as
mechanical ventilatoras or diaphragmatic pace makers
Complete SCI leads to…
Neurologic deficit below site of injury
-Quadruplegia ( tetraplegia)
-paraplegia
Permanent paralysis
Goals of Rehabilitation
* Educate patient and family about SCI
* Maximise proficiency with mobility and self care
* Teach appropriate bowel and bladder management
* Prevent co-morbidities (contractures, skin break downs) associated
with SCI Assess psychological well being and initiate community and
vocational re-intergration to society.
Calcium has surprising role in sensing pain
When you accidentally touch a hot oven, you rapidly pull your hand
away. Although scientists know the basic neural circuits involved in
sensing and responding to such painful stimuli, they are still sorting
out the molecular players. Duke researchers have made a surprising
discovery about the role of a key molecule involved in pain in worms,
and have built a structural model of the molecule. These discoveries may
help direct new strategies to treat pain in people.
In humans and other mammals, a family of molecules called TRP ion
channels plays a crucial role in nerve cells that directly sense painful
stimuli.
 Researchers are now blocking these channels in clinical trials to
evaluate this as a possible treatment for various types of pain. Researchers are now blocking these channels in clinical trials to
evaluate this as a possible treatment for various types of pain.
The roundworm Caenorhabditis elegans also expresses TRP channels -
one of which is called OSM-9 - in its single head pain-sensing neuron
(which is similar to the pain-sensing nerve cells for the human face).
OSM-9 is not only vital for detecting danger signals in the tiny worms,
but is also a functional match to TRPV4, a mammalian TRP channel
involved in sensing pain.
In the new study, researchers created a series of genetic mutant
worms in which parts of the OSM-9 channel were disabled or replaced and
then tested the engineered worms’ reactions to overly salty solution,
which is normally aversive and painful.
Specifically, the mutant worms had alterations in the pore of the
OSM-9 channels in their pain-sensing neuron, which gets fired up upon
channel activation to allow calcium and sodium to flow into the neuron.
That, in turn, was thought to switch on the neural circuit that encodes
rapid withdrawal behaviour - like pulling the finger from the stove.
“People strongly believed that calcium entering the cell through the
TRP channel is everything in terms of cellular activation,” said lead
author Wolfgang Liedtke, an associate professor of neurology at Duke
University School of Medicine. With then-graduate student Amanda Lindy,
“we wanted to systemically mutagenise the OSM-9 pore and see what we
could find in the live animal, in its pain behaviour,” Liedtke said.
To the group's surprise, changing various bits of OSM-9's pore did
not change most of the mutant worms’ reactions to the salty solution.
However, these mutations did affect the flow of calcium into the cell.
The disconnect they saw suggested the calcium was not playing a direct
role in the worms’ avoidance of danger signals.
Calcium has been thought to be indispensable for pain behaviour - not
only in worms’ channels but in pain-related TRP channels in mammals.
So results from the engineered OSM-9 mutant worms will change a
central concept for the understanding of pain, Liedtke said.
To see whether calcium might instead play a role in the worms’
ability to adapt to repeated painful stimuli, the group then repeatedly
exposed pore-mutant worms to the aversive and pain stimuli.
After the tenth trial, a normal worm becomes less sensitive to high
salt. But one mutant worm with a minimal change to one specific part of
its OSM-9 pore - altered so that calcium no longer entered but sodium
did - was just as sensitive on the tenth trial as on the first.
The results confirmed that calcium flow through the channel makes the
worms more adaptable to painful stimuli; it helps them cope with the
onslaught by desensitising them. This could well represent a survival
advantage, Liedtke said.
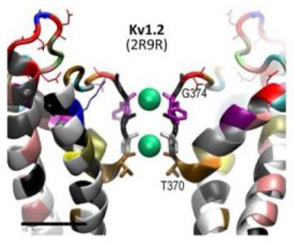
To put the findings into a structural context, Liedtke collaborated
with computational protein scientists Damian van Rossum and Andriy
Anishkin from Penn State University, who built a structural model of
OSM-9 that was based the recently resolved structure of TRPV1, the
molecule that senses pain caused by heat and hot chilli peppers.
The team was then able to visualise the key parts of the OSM-9 pore
in the context of the entire channel. They understood better how the
pore holds its shape and allows sodium and calcium to pass.Liedtke said
that understanding this structure could be a great help in designing
compounds that will not completely block the channel but will just
prevent calcium from entering the cell.
- MNT |













")

