|

Understanding haemophilia
By Carol Aloysius
Haemophilia is a rare bleeding disorder which is still not understood
completely by even many medical professionals, let alone the lay public.
Although the cure for this disease is still at an experimental stage,
understanding the disease and proper patient care by the whole family
will help to relieve the suffering of the patient and give them a better
future. On April 17 World Haemophilia Day 2013 was observed with The CN
Tower, one of the world's tallest freestanding structures, lit up in red
to mark this event and raise awareness about this little known genetic
bleeding disorder.
 Consultant Haematologist of National Hospital of Sri Lanka, Colombo,
Dr. Bhaddika Rasanjalie Jayaratne talks about the disease and briefly
traces its origins in a recent interview with the Sunday Observer. Consultant Haematologist of National Hospital of Sri Lanka, Colombo,
Dr. Bhaddika Rasanjalie Jayaratne talks about the disease and briefly
traces its origins in a recent interview with the Sunday Observer.
Excerpts...
Q. What is haemophilia? How is it caused?
A. Haemophilia is a group of inherited blood disorders in
which the blood does not clot properly. Blood contains many proteins
called clotting factors including factor VIII and factor IX, which
maintain at constant levels and work to stop bleeding through complex
chemical interactions. People with haemophilia have a low level or
absence of one of these clotting factors in blood. Haemophilia A and B
are caused by deficiency of clotting factors, factor VIII and factor IX
respectively and not surprisingly their absence causes virtually
identical patterns of bleeding. The existence of lifelong bleeding
disorders and their familial occurrence was noted in the medical
literature as early as the 16th century.
Haemophilia figured prominently in the history of European royalty in
the 19th and 20th centuries. Britain's Queen Victoria, through two of
her five daughters, passed the mutation to various royal houses across
the continent, including the royal families of Spain, Germany and
Russia.
Q. How is it transmitted?
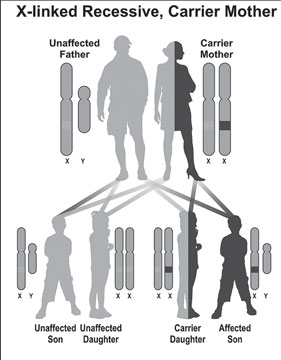
A. The disease is transmitted from parents to children through
non-dominant Haemophilia gene located on chromosome X. Females possess
two X chromosomes. Males have one X and one Y chromosome.
Therefore, a vast majority of patients are males and females are
asymptomatic carriers, but there are very rare cases of female
haemophilia patients reported in certain tribes of south India. About
one-third of patients may not have a prior family history.
Blood contains many proteins called clotting factors including factor
VIII & factor IX, which maintain at constant levels and work to stop
bleeding through complex chemical interactions.
The disease is transmitted from parents to children through
non-dominant Haemophilia gene located on chromosome X. Females possess
two X chromosomes.
Males have one X and one Y chromosome. Therefore, a vast majority of
patients are males and females are asymptomatic carriers, but there are
very rare cases of female haemophilia patients reported in certain
tribes of south India. About one-third of patients may not have a prior
family history.
Q. Who is at risk of inheriting this condition?
A. People with haemophilia have a low level or absence of one
of these clotting factors in blood. Haemophilia A and B are caused by
deficiency of clotting factors, factor VIII and factor IX and not
surprisingly their absence causes virtually identical patterns of
bleeding.
Haemophilia A affects approximately 1 in 10 000 live male births and
is equally common in all ethnic groups whereas Haemophilia B incidence
recorded approximately 1 in 50,000 male births around the world.
According to world haemophilia federation statistics the total number
of Haemophilia patients in the world is recorded as 400,000 in 2012.
There are 316 haemophilia patients registered at National Hospital
Colombo to date, out of which 276 are haemophilia A.
Q. What are the symptoms?
A. The characteristic symptoms vary with severity. In general
symptoms are internal or external episodes of bleeding. Patients with
severe haemophilia suffer spontaneous, frequent and severe bleeds and
patients with mild haemohilia suffer minor symptoms. In fact mothers
notice frequent, large bruises and swelling of knee joints when their
sons start crawling or bleeding from a dental procedure, following
trauma or surgery as a first sign.
The most characteristic type of internal bleed is joint bleeding.
Bleeding into subcutaneous tissue and muscle is also seen. Less commonly
but life threatening gastrointestinal, central nervous system and
bleeding into genitourinary system are also experienced. Long term
complications include, joint, muscle deformities, 'pseudotumour
formation' and fractures.
Out of all it has to be considered that the quality of lives of these
patients are affected in many ways with regard to their socio-economic,
psychological conditions and family lives. Frequent hospital admissions,
absence at school and work, being dependent on their family members and
society are also consequences of the disease process.
Q. What are the services available to patients in Sri Lanka?
A. In Sri Lanka, state sector health services play a major
role in caring haemophilia patients at recognised centers involving full
array of laboratory diagnosis, factor replacement therapy for acute
symptoms and prevention of further bleeding under supervision of
comprehensive care team including a haematologist, physician, dentist,
physiotherapist, counsellor and social worker.
Factor replacement therapy is exclusively available in the state
sector hospitals at specialised centres which are substantially a costly
treatment. Approximately a minimum of Rs 30,000 Sri Lankan rupees is
spent for management of an uncomplicated joint bleed in hospital, per
day.
This is where a calculated level of factor VIII or factor IX
replacement on regular basis for the purpose of prevention of recurrent
bleeding comes in not only to minimise the cost bore by the government
and also to improve the quality of life of patients to live a near
normal life.
Unfortunately the currently available plasma derived factor treatment
rarely carries a risk of plasma transmitted infections such as Hepatitis
B and development of resistance to treatment.
Q. Is there a cure for this disease?
A. There is no cure for this genetic disease except gene
therapy which is still at an experimental level.
Caring haemophilia patients is an equally shared responsibility of
their immediate family members, relatives and the society at school,
workplace and public in general.
These patients have to be treated equally with other unaffected
siblings within their families while more attention, care and love are
expected. Their parents and immediate family members should have an
understanding regarding nature of the illness, identification of early
symptoms, to obtain appropriate medical treatment as early as possible
when necessary.
Q. What advice do you have for parents and teachers of
children with haemopholia?
A. Haemophilia patients at school may need help from the
teachers and their friends whenever it is necessary and also need more
attention at physical activities.
High contact sports such as soccer, hockey and rugby are not suitable
for them whereas swimming, table tennis, badminton, cycling, rowing and
chess are safe. If the child develops symptoms at school they should
direct him to hospital immediately and inform the parents.
Q. Do children with haemophiolia have a lower IQ than normal
children?
A. Children with haemophilia are intellectually equal with
their peers and should, therefore, not be discriminated against. At work
the colleagues and the superiors also should have an understanding about
their condition and be able to offer a supporting hand whenever
necessary.
They should not be occupied in more strenuous physical engagements
which carry risk of bleeding.
In their day to day routine in public places, the road, at
supermarkets, religious places and public transport, the public should
also care another member of their society if a necessity arises to help
him. Everybody has a responsibility in the society to live with healthy
hygienic habits mostly inculcated by their traditions and culture.
Q. Your advice on any other special health risks that such
patients face?
A. Haemophilia patients in particular should be responsible in
living in correct hygienic routine including special dental care to
prevent getting dental caries, and also rushing to the nearest hospital
where Haemophilia care is available at the very beginning of symptoms,
what they called 'aura.' Attending clinics, regular dental checkups and
receiving scheduled vaccinations at appropriate times are also part of
their responsibility.
Available and possible genetic testing should be offered to, at risk
female family members of haemophilia patients to facilitate making more
informed choices regarding future pregnancies and prenatal diagnosis.
However termination of pregnancy due to affected haemophilia foetus
is still not legalised in Sri Lanka.
The Haemophilia Association of Sri Lanka is founded in year 2000 and
is a 500-member society to date, which raises a voice for each and every
individual haemophilia patient in Sri Lanka with a link to World
Haemophilia Federation. However, haemophilia is a lifelong disabling
disease which has no cure other than factor replacement and preventive
or supportive care.
These members of our society are intellectually normal and live
courageously with us, contributing in many ways to the country's economy
through all walks of life; in fact some of them are outstanding
professionals, artists, businessmen, students and even sports personnel.
Let us salute them for their courage to live despite all hardships
that they face in the course of events in life.
Only five percent wash hands correctly
Remember Mom's advice about washing your hands thoroughly after using
the restroom? Apparently not.
A new study found that only five percent of people who used the
bathroom washed their hands long enough to kill the germs that can cause
infections.
 What's more, 33 percent didn't use soap and 10 percent didn't wash
their hands at all. Men were particularly bad at washing their hands
correctly. What's more, 33 percent didn't use soap and 10 percent didn't wash
their hands at all. Men were particularly bad at washing their hands
correctly.
The study, based on observations of 3,749 people in public restrooms,
appears in the Journal of Environmental Health. "These findings were
surprising to us because past research suggested that proper hand
washing is occurring at a much higher rate," said Carl Borchgrevink,
associate professor of hospitality business and lead investigator on the
study. Hand washing is the single most effective thing one can do to
reduce the spread of infectious diseases, according to the Centres for
Disease Control and Prevention. Failing to sufficiently wash one's hands
contributes to nearly 50 percent of all food-borne illness outbreaks It
takes 15 to 20 seconds of vigorous hand washing with soap and water to
effectively kill the germs, the CDC says, yet the study found that
people are only washing their hands, on average, for about 6 seconds.
Borchgrevink and colleagues trained a dozen college students in data
collection and had them observe hand washing in restrooms in bars,
restaurants and other public establishments. The student researchers
were as unobtrusive as possible - by standing off to the side and
entering results on a smart phone, for example. The study is one of the
first to take into account factors such as duration of the hand washing
and whether people used soap.
Specific findings include:
- Fifteen percent of men didn't wash their hands at all, compared
with seven percent of women.
- When they did wash their hands, only 50 percent of men used soap,
compared with 78 percent of women.
- People were less likely to wash their hands if the sink was dirty.
- Hand washing was more prevalent earlier in the day. Borchgrevink
said this suggests people who were out at night for a meal or drinks
were in a relaxed mode and hand washing became less important.
- People were more likely to wash their hands if a sign encouraging
them to do so was present.
Borchgrevink, who worked as a chef and restaurant manager before
becoming a researcher, said the findings have implications for both
consumers and those who operate restaurants and hotels.
"Imagine you're a business owner and people come to your
establishment and get food-borne illness through the faecal-oral route -
because people didn't wash their hands - and then your reputation is on
the line," he said. "You could lose your business."
- Medicalxpress
Professional women more susceptible to breast cancer
Successful women may be more likely to develop breast cancer - and
stress at work, including prejudice, discrimination, and resistance,
could be to blame. Women in professional jobs had a near 70 percent
higher risk of breast cancer than other women, according to new
research.
|
Breast screening |
The research, based on a 55-year study of women who were in their
thirties in the 1970s, links job stress and cancer, and shows that the
longer a woman held the job, the greater the risk. The researchers say
that while women going into management in the 1970s were breaking new
ground, the same kind of stress affects women today.
"Women who entered managerial occupations in the 1970s experienced
prejudice and discrimination due to prevailing cultural attitudes that
men made better leaders than women,'' says Dr Tetyana Pudrovska, who led
the study. "Neither men or women preferred to work for a woman because
women were seen as "temperamentally unfit" for management, which was
consistent with the cultural stereotype of the woman boss.
"Exercising job authority was particularly stressful for women in the
context of gender inequality embedded in the occupational structure of
the time, when women in managerial positions often faced prejudice,
tokenism, discrimination, social isolation, and resistance from
subordinates, colleagues, and superiors. We believe that women are still
facing the same kind of stresses, and therefore the increased risk is
likely to be there...today."
The study focused on nearly 4,000 women who were all aged 36 in 1975.
-The Independent
Diabetes diagnosed through cheaper methods
Diabetes patients often receive their diagnosis after a series of
glucose-related blood tests in hospital settings, and then have to
monitor their condition daily through expensive, invasive methods. But
what if diabetes could be diagnosed and monitored through cheaper,
noninvasive methods?
Chemists at the University of Pittsburgh have demonstrated a sensor
technology that could significantly simplify the diagnosis and
monitoring of diabetes through breath analysis alone. Their findings
were published in the latest issue of the Journal of the American
Chemical Society (JACS).
 Even before blood tests are administered, those with diabetes often
recognise the condition's symptoms through their breath acetone - a
characteristic "fruity" odor that increases significantly with high
glucose levels. The Pitt team was interested in this biomarker as a
possible diagnostic tool. Even before blood tests are administered, those with diabetes often
recognise the condition's symptoms through their breath acetone - a
characteristic "fruity" odor that increases significantly with high
glucose levels. The Pitt team was interested in this biomarker as a
possible diagnostic tool.
"Once patients are diagnosed with diabetes, they have to monitor
their condition for the rest of their lives," said Alexander Star,
principal investigator of the project and Pitt associate professor of
chemistry. "Current monitoring devices are mostly based on blood glucose
analysis, so the development of alternative devices that are
noninvasive, inexpensive, and provide easy-to-use breath analysis could
completely change the paradigm of self-monitoring diabetes."
Together with his colleagues - Dan Sorescu, a research physicist, and
Mengning Ding, a Pitt graduate student studying chemistry - Star used
what's called a "sol-gel approach," a method for using small molecules
(often on a nanoscale level) to produce solid materials. The team
combined titanium dioxide - an inorganic compound widely used in
body-care products such as makeup - with carbon nanotubes, which acted
as "skewers" to hold the particles together. These nanotubes were used
because they are stronger than steel and smaller than any element of
silicon-based electronics.
This method, which the researchers playfully call "titanium dioxide
on a stick," effectively combined the electrical properties of the tubes
with the light-illuminating powers of the titanium dioxide. They then
created the sensor device by using these materials as an electrical
semiconductor, measuring its electrical resistance (the sensor's
signal). The researchers found the sensor could be activated with light
to produce an electrical charge. This prompted them to "cook" the
"skewers" in the sensor under ultraviolet light to measure acetone
vapors - which they found were lower than previously reported
sensitivities.
"Our measurements have excellent detection capabilities," said Star.
"If such a sensor could be developed and commercialised, it could
transform the way patients with diabetes monitor their glucose levels."
The team is currently working on a prototype of the sensor, with
plans to test it on human breath samples soon.
-MNT |










")



