|

Vector diseases infect 1 billion, kills over 1
million worldwide:
Small bite, big threat
By Carol Aloysius
More than half the world's population is at risk from diseases such
as malaria, dengue, leishmaniasis, Lyme disease, schistosomiasis, and
yellow fever, carried by mosquitoes, flies, ticks, water snails and
other vectors.
Every year, more than one billion people are infected and more than
one million die from vector-borne diseases. Because of the serious and
increasing threat of such diseases on human lives, World Health Day
(April 7) was marked by a renewed focus and call for global action
against vector borne diseases, with the slogan “Small bite, big threat”.
Most importantly was the message it underlined: these diseases are
entirely preventable.
As Dr Margaret Chan, WHO Director General says, “Simple,
cost-effective interventions like insecticide-treated bed nets and
indoor spraying have already saved millions of lives. “No one in the
21st century should die from the bite of a mosquito, a sand fly, a black
fly or a tick.”
Consultant Microbiologist at Sri Jayawardenepura Hospital Dr Kushlani
Jayatilleke draws from her hands-on experience to give new insights on
risks that Lankans face from the common vectors found here.
|

The mosquito is the vector responsible for transmitting most
diseases. Dengue and Chikungunya are transmitted by Aedes
aegypti and Aedes albopictus. |
Excerpts from an interview with the Sunday Observer...
Q. World Health Day this year decided to focus on vector borne
diseases. Is there a sudden surge in such diseases?
A. More than half of the world's population is at risk from
vector-borne diseases such as malaria and dengue.
Q. Explain in laymen language what a vector is and how it can
cause a disease in human beings. Is it a germ? A virus? A bacteria?
A. A vector is a living organism, often an invertebrate
arthropod, that transmits a pathogen and thus an infectious disease from
reservoir to host. In simple terms it is an insect that carries a virus,
a protozoa, a bacterium, or any other parasite which can cause diseases,
to a human from another human or an animal.
Q. What are the most common vector diseases globally?
A. According to the latest estimates, released in December
2013, there were about 207 million cases of malaria in 2012 (with an
uncertainty range of 135 million to 287 million) and an estimated
627,000 deaths (with an uncertainty range of 473,000 to 789,000). Over
2.5 billion people - over 40 percent of the world's population - are now
at risk from dengue. WHO currently estimates there may be 50-100 million
dengue infections worldwide every year.
Nearly 1.4 billion people in 73 countries worldwide are threatened by
lymphatic filariasis, Over 120 million people are currently infected,
with about 40 million disfigured and incapacitated by the disease.
An estimated 1.3 million new cases of leishmaniasis occur annually.
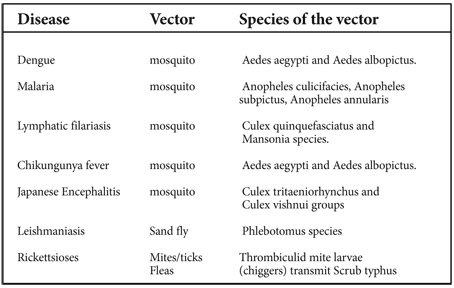
Q. What about Sri Lanka? What are the common vector borne
diseases found here? Dengue? Filaria? Malaria? Others ?
A. Dengue is the most common vector borne disease in Sri
Lanka, today. Japanese Encephalitis, Chikungunya fever, lymphatic
filariasis, Leishmaniasis, Rickettsioses and malaria are the other
vector borne diseases reported.
Q. Are they endemic diseases? Or do they occur just once in a
while?
A. Dengue is endemic in Sri Lanka. Locally transmitted malaria
has not been reported from Sri Lanka since October 2012.
Lymphatic filariasis is endemic in eight districts in three provinces
(Western, Southern and North Western Provinces). Reaching the stage of
elimination of lymphatic filariasis from Sri Lanka. Chikungunya fever,
and Japanese Encephalitis occur as outbreaks. Leishmaniasis,
Rickettsioses are being reported as sporadic cases.
Q. Which vector causes most of these diseases? Is it the
mosquito? If so what species of mosquitoes are responsible for
transmitting them?
2. A. The mosquito is the vector responsible for transmitting most of
these diseases. Dengue and Chikungunya are transmitted by Aedes aegypti
and Aedes albopictus.
Q. Of the diseases you mentioned, which of them have become
diseases of the past?
A. The malaria and Lymphatic filariasis disease burden has
come down significantly during the past few years. In malaria, no new
indigenous cases are reported at present and only few imported cases are
reported.
Q. How did this happen? Better and quicker detection methods?
Awareness raising, or an integrated approach to the issue?
A. This was through integrated approach through the dedicated
“National Malaria Control Program of Sri Lanka” and through the “Anti
Filariasis Campaign”.
Q. As a microbiologist what is your role in early detection of
these diseases?
A. As a Microbiologist I have to help clinicians to diagnose
these diseases by suspecting them in patients and requesting the correct
investigations. Also, I have to make the relevant investigations
available in the laboratories where I work.
For some diseases such as Leishmanasis, special input on management
and treatment is also necessary.
Q. Dengue is currently widely prevalent in this country. But
the Health Ministry insists the numbers of cases have dropped.
A. If we look at the trends of dengue in the past few years,
we can see that the number of cases has decreased in the first few
months of each year. In keeping with this trend the numbers have come
down in the first few months of 2014 as well. Also we can see that the
2014 numbers are lower than the numbers we had in the first few months
of 2010, 2012 and 2013.
But the more dramatic impact is on the mortality rate or the
proportion of patients who die of dengue. This has come down drastically
during past few years due to the proper management of patients according
to guidelines.
Q. I'm told there are four different species of mosquitoes[u1]
that cause dengue. Is this correct? What are they?
A. Four serotypes of dengue virus are recognised and
correspond to four distinct virus species (dengue-1 to dengue-4) based
on antigenic and genetic characteristics.
Q. Which of these species exist in Sri Lanka ?All of them? Are
they seasonal? If so which of them are more widely prevalent at this
time of the year (March, April-May ?)
A. All four types have been reported in Sri Lanka. Dengue
virus serotypes 2 and 3 were the predominant circulating serotypes until
2009 and were responsible for 86 percent of dengue infections. Dengue 1
serotype only accounted for 7 percent of infections. PCR results of
patients with DHF recruited from August 2010 to December 2010 showed
that dengue 1 serotype accounted for more than 95 percent of dengue
infections. All dengue virus serotypes have been associated with severe
clinical disease.
Q. How does a microbiologist isolate the kind of species that
are more prevalent at a specific time of the year? What are the tools
you use? Do weather conditions and climate count?
A. Virus isolation is not performed in routine clinical
laboratories. The virus isolation and Nucleic acid detection reverse
transcriptase polymerase chain reaction (RT-PCR) need a sophisticated
laboratory.
Q. Are these techniques available in all hospitals (state and
private) in the country?
A. Dengue non-structural protein 1 (NS1) antigen detection
kits and Dengue IgM antibody detection kits are available in major
hospitals only. The dengue IgM antibody is detectable in blood only
after 4-5 days of fever. The NS1 antigen is detectable in the serum of
dengue virus infected patients as early as one day after developing the
fever and up to 18 days after onset.
Q. What is needed to confirm whether a patient suspected of
dengue has got the disease or not? A blood specimen? Platelet count?
A. A full blood count is recommended in patients who have
fever for three days. This will give the platelet count as well as the
white blood cell count. Haematocrit is another good indicator. The
confirmation of dengue viral infection has to be done by NS1 antigen
test or any other test mentioned above. This is not necessary for
clinical management of the patient.
Q. Where should he go for these tests? Are they available at
all hospitals? Are they free of charge?
A. Full blood count is available in most of the Base and
General Hospitals in the country free of charge and in most private
sector laboratories for a fee.
Q. What would you say is the current range in the prices
charged by a private or semi government hospital for such tests compared
to the free tests in a state hospital?
A. The price will range from Rs. 300/= to 500/=.
Q. Since dengue is the most widely prevalent disease right
now, tell me who are those most at risk of getting it? Children (what
age groups), adolescents? Adults? Elderly? Why?
 A. Dengue has been reported in every age group from new born
babies to elderly, but severe dengue (also known as dengue haemorrhagic
fever) which is characterised by fever, abdominal pain, persistent
vomiting, bleeding and breathing difficulty and is a potentially lethal
complication, affects mainly children. A. Dengue has been reported in every age group from new born
babies to elderly, but severe dengue (also known as dengue haemorrhagic
fever) which is characterised by fever, abdominal pain, persistent
vomiting, bleeding and breathing difficulty and is a potentially lethal
complication, affects mainly children.
Q. Our hospitals are overflowing with children including
babies suspected of having the dengue virus? Your comments?
A. Yes, especially during the season when more dengue cases
are reported most of the hospital medical wards are overflowing with
dengue patients.
Q. To confirm their suspicions doctors often order a platelet
test? What is it ? What is required of the person for this test? If done
outside a state hospital what is the cost?
A. It is a simple blood test which costs around Rs 500/= or
less.
Q. When should this test be done to be hundred percent
accurate?
A. It should be done on the fourth day of fever as in most
patients with dengue this is the time the platelets will start dropping.
But in pregnant patients and in other immuno-compromised patients this
should be done even before that.
Q. What are the symptoms that indicate his condition?
A. Dengue should be suspected when high fever (1040F) is
accompanied by two of the following symptoms; severe headache, pain
behind the eyes, muscle and joint pains, nausea, vomiting, swollen
glands or rash.
Q. Can dengue be prevented with drugs? A vaccination ?
A. No. At present there is no vaccine or drug that can prevent
dengue.
Q. Can the flu shots taken in other countries and now
introduced to Sri Lanka in a limited way prevent one getting the
disease? If so, for how long is the period of immunity?
A. A flu shot is to protect you from influenza. It is not
effective in preventing dengue infection.
Q. Once a person gets dengue can it recur?
A. Yes. As there are 4 serotypes, re-infection can occur with
another sero-type.
Q. Is it true that the first attack of dengue is usually the
most severe. Why?
A. Usually the first attack is mild and subsequent attacks are
more severe. This is because the immune response actually makes the
clinical symptoms of dengue worse, increasing the risk of severe dengue.
Q. What are the Do's and Don'ts for a person suspected of a
drop in his platelet count of having dengue? Should he take paracetamol
or any other medication to cause the fever to go down?
Do's
1. Take adequate bed rest
2. Drink enough fluid such as oral rehydration solution (ORS), fruit
juice and other fluids containing electrolytes and sugar to replace
losses from fever and vomiting. Adequate oral fluid intake may be able
to reduce the number of hospitalisations
3. Paracetamol can be taken for fever and body aches. The interval of
paracetamol dosing should not be less than six hours. Tepid sponge if
the patient still has high fever.
4. After three days of fever or if the patient is pregnant or
immune-compromised before that, see a doctor.
5. The patient should be brought to hospital immediately if any of
the following occur:
* no clinical improvement,
* deterioration when fever comes down
* severe abdominal pain
* persistent vomiting
* pale, cold, clammy hands and feet
* lethargy or irritability/restlessness
* drowsiness, mental confusion or seizures
* bleeding (e.g. black stools, coffee-ground vomiting, red spots or
patches on the skin, bleeding from nose or gums, vomiting blood, black-coloured
stools, heavy menstruation/vaginal bleeding)
* Not passing urine for more than 4-6 hours.
* Difficulty in breathing
Don'ts
1. Do not take aspirin and other anti-inflammatory drugs such as
ibuprofen, indomethacin or voltaren.
2. Do not drink dark coloured drinks such as coffee or coke or eat
red coloured food such as beetroot.
3. Antibiotics are not necessary.
Q. What about cross infection in hospitals? Do you think most
parents will be better off keeping their kids and treatment or observing
them at home before bringing them to the hospital straightaway?
A. As I explained before if fever persists after 3 days they
should see a qualified doctor. The doctor should assess the patient and
decide whether the patient can be managed at home or need admission to
hospital.
Q. Has there been any new breakthrough in 1) detecting dengue
early 2) treating it? Is gene technology one of them?
A. Detecting dengue, especially severe form of dengue early
along with proper clinical management is the key to reduce deaths from
dengue. NS1 antigen detection is a simple test that can be done in
routine laboratories and which detects dengue virus infection early.
Q. What are the health impacts of dengue and other vector
borne diseases on humans?
A. As discussed above dengue and other vector borne disease
can cause deaths as well as loss of productivity in young patients,
including children.
Q. Your message to the public?
A. We all have a responsibility in controlling vector borne
diseases. Dengue prevention and control solely depends on effective
vector control measures.
As the dengue mosquito lives in urban habitats and breeds mostly in
man-made containers all of us have a role to play in controlling this
mosquito. Check in your homes where water is collected and clean and
empty them as often as possible. Change the water in flower vases and
other ornamental water containing equipment.
Keep the environment clean so that water is not collected in small
containers or polythene bags etc. Look for small holes and pits where
water can get collected and close them. Unlike other mosquitoes, Ae.
aegypti is a daytime feeder; its peak biting periods are early in the
morning and in the evening before dusk.
Female Aedes aegypti bites multiple people during each feeding
period. Therefore keep the doors and windows closed during dawn and dusk
and have mosquito proof mesh fixed on the grills and other openings of
homes.
When going outdoors, and when children are playing outdoors, a
mosquito repellent can be applied to prevent mosquito bites.
Good oral care should last a lifetime
by Dr Irosha R. Perera
Oral health care is a very important factor for a healthy lifestyle,
general health and well-being throughout the world. Good oral health
care should be practiced throughout life, starting as early as when a
mother is pregnant with the child. In fact, it should form a part of our
daily routine and should be given priority. When a pregnant woman has
bad oral health, she can't take antibiotics and different tests such as
radiological investigations like x-rays freely. If she's having cavities
it will affect the future of the child's oral health as well. When the
mother carries cavity forming bacteria, the baby is more likely to get
cavities as well.
Bacteria
Fluoride containing toothpaste is a must and is recommended by
dentists. The acid formed by bacteria ruins the enamel, resulting in
cavities. Normally, the saliva neutralises the bad effects, but there's
a limit and an extent to which it can neutralise.
 If the mouth pH level is below 5.5 ,de-mineralisation of the minerals
(dissolving of calcium and phosphate from the tooth) starts take place. If the mouth pH level is below 5.5 ,de-mineralisation of the minerals
(dissolving of calcium and phosphate from the tooth) starts take place.
With the use of fluoridated toothpaste, the fixing effect happens
where the fluoride re-mineralises the de-mineralised teeth, resistant to
the acid affect and ensures that a protective action around the tooth.
Even in the areas of high levels of fluoride in water where people
drink and use highly fluoridated water for cooking, it is advised to use
fluoridated toothpaste when brushing. Fluoridated toothpaste can help us
re-mineralise the de-mineralized enamel. Demineralised early caries
lesion, chalky white spots on the surface of the tooth, which is the
first stages of cavity, can be easily detected close to gum margins of
tooth surface in children with milk teeth.
Brushing
Brushing the children's teeth with fluoridated toothpaste twice a
day, brushing the gum margins and in between teeth thoroughly is
important to ensure oral health and freedom from cavities. It is also
important to ensure that treats such as sweets, bubblegum, biscuits and
sweet drinks are minimised. The fluoridated toothpaste will also
strengthen the enamel and control cavities and gum diseases since it is
also anti-bacterial. About 30 percent of the adults and 50 percent of
the children do not brush with fluoridated toothpaste before going to
bed but responds otherwise when questioned in surveys - this is called
social desirability response bias.
Social inequality and poverty plays a great role in widening
disparities in oral health, which places a burden on the health systems
of countries such as Sri Lanka.
People with diabetes and periodontal disease (gum disease) need to
clean their teeth with fluoridated toothpaste - bacteria and gum disease
can disturb the glycemic control and diabetes increases the severity of
gum disease causing a two way reaction. Brushing their teeth twice a day
with fluoridated toothpaste and of course with a brush with softer
bristles will help them keep their teeth clean and safe. Caries and gum
disease can be prevented and controlled if you use the proper strategies
- namely using fluoride toothpaste, deploying a proper way of brushing
and ensuring the intake of a healthy diet. Visiting the Dentist for
check ups once in six months would also make things better.
The writer is Dental Public Health Specialist, Preventive Oral Health
Unit/Community Dental Unit, Dental Institute, Colombo |














")